Download
1 / 33
760 likes | 2.01k Views
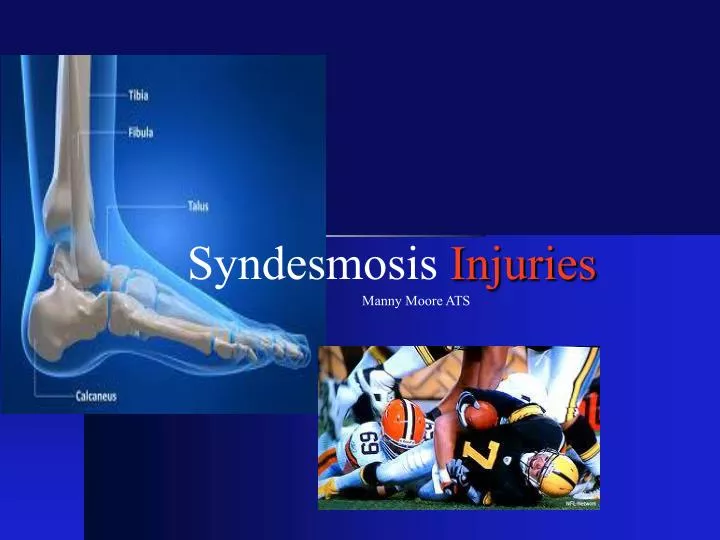
Syndesmosis Injuries. Manny Moore ATS. Syndesmosis Injuries. 11-18% of all ankle sprains Longer recovery v.s. Lateral sprains Men v.s. Women?. Bone Anatomy. Tibia Articular Surface Fibula Articular Surface Talus Dome. Provides Stability & Proper Ankle Function .

E N D
Syndesmosis Injuries Manny Moore ATS
Syndesmosis Injuries 11-18% of all ankle sprains Longer recovery v.s. Lateral sprains Men v.s. Women?
Bone Anatomy • Tibia Articular Surface • Fibula Articular Surface • Talus Dome Provides Stability & Proper Ankle Function Articular Surface
Snydesmosis Ligaments • AIFL- Chaput’s Tubercle Most Vulnerable • PIFL- Wagstaffe’s Tubercle Strongest • ITFL- Thickening of PIFL • IM- Fibrous tissue Transmit force • IL- Thickening of IM
Biomechanics • Mechanism of Injury Eversion Dorsiflexion Pronation • Closed Pack Position Forces the talus against the fibula Widening of mortise 1mm lateral shift increases joint surface pressure by 42% Associated injuries?
Clinical Examination • History ER with DF Contact None Contact Acute v.s. Chronic • Observation Edema Eccymosis Antalgic gait Possible Deformity?
Clinical Examination • Palpation • Tenderness Length Nussbaum et al. • Special Test Squeeze Test Dorsiflexion Test Kleigers Test Cross-leg Test
Imaging Techniques X-RAY • Radiographs • AP, Lateral, Mortise Views • AP View • Fractures • Tibiofibular clear space widening of 6 mm • Tibiofibular overlap > 42% Fibula Width • Medial clear space widening > 4mm • Lateral View • Non weight bearing ER • Fractures
Imaging Techniques X-RAY Tibiofibula overlap Tibiofibula clearance space Medial clear space
Imaging Techniques X-RAY Tibiofibula overlap Tibiofibula clearance space Medial clear space
Imaging Techniques X-RAY • Lateral View
Imaging Techniques X-RAY • AP View Heterotopic Ossification
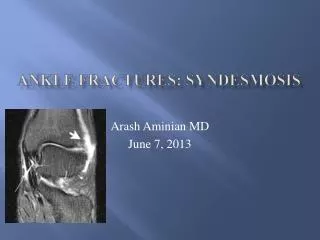
Imaging Techniques MRI & CT • MRI (Magnetic Resonance Imaging) • Frontal, Axial, Saggital Views High sensitivity and specificity More reliable detecting disruptions • CT (Computed Tomography) More effective detecting minor disruptions Less Cost v.s. MRI
Imaging Techniques MRI • Axial Views
West PointInstability Scale Grade I Grade II Grade III
Conservative Non Conservative TreatmentCriteria Based on Patients Goals Length of Symptoms Severity of Injury Grade I Non-Fractures Stable Grade II Grade III Unstable Grade II Fractures Chronic Injury
ConservativeProtocols • Results vary patient to patient • Grade I Injuries: 2-4 Weeks RTP • Grade II Injuries: 6-8 Weeks RTP WithoutInstability or Fractures
ConservativeProtocols • Phase I (0-5 Days) or (5-14Days) • Immobilize • Reduce Pain • Reduce Inflammation • Cryotherapy • E-Stim • Increase ROM • Manual 30* PF Stretch • Ankle Pumps • Toe Curls • Towel Stretch
ConservativeProtocols • Phase II (6-10 Days) or (2-4 weeks) • Immobilize Grade II • Reduce Pain • Reduce Inflammation • Proprioception • Increase Flexibility • Increase ROM • Increase Strength • CV Endurance
ConservativeProtocols • Phase III (18-25 Days) or (4-8 Weeks) • Protect Injury • Reduce Pain • Increase Pain free Activity • Sports Specific • Proprioception • Increase Strength • Increase Flexibility • CV Endurance
ConservativeProtocols • Phase III (18-25 Days) or (4-8 Weeks) • Sports Specific Drill#2 Drill#1
ConservativeProtocols Return To Play Criteria • Full Strength • Full ROM • Functional Test • Physician Clearance • Protect Injury
Operative Treatment Arthroscopy • Goal is to restore structures, and mobility • Open Reduction & Internal Fixations • Autographs • Modified Brostrum Technique • 4.5 mm Cortical Screws • Complications • Screw Breakage • Screw Type • Infection • Calcification & Joint Stiffness
Operative Treatment Arthroscopy Before After
Post-Operative Protocols Arthroscopy • Results vary patient to patient • Grade III Injuries: 4-8 Months RTP • Non Weight Bearing 6-8 Weeks • Screw Removal @ 3 Months • Follow-up Imaging every 2 weeks
Post-Operative Protocols • Phase I (1-3 Weeks) • Phase I- Conservative Rehabilitation • Immobilize & Non Weight Bearing • Protect Wound • Reduce Pain • Reduce Inflammation • Proprioception • Increase ROM • Maintain Flexibility • CV Endurance
Post-Operative Protocols • Phase II (3-8 Weeks) • Phase I- Conservative Rehabilitation • Immobilize & Partial Weight Bearing • Protect Wound • Reduce Pain • Reduce Inflammation • Increase ROM • Increase Strength • Proprioception • Increase Flexibility • CV Endurance
Post-Operative Protocols • Phase III (8-12 Weeks) • Phase II- Conservative Rehabilitation • Full Weight Bearing & Cam-walker • Remove Screws • Reduce Pain • Increase ROM • Increase Strength • Proprioception • Increase Flexibility • Sports Specific • CV Endurance
Post-Operative Protocols • Phase IV (4-8 Months) • Phase III Conservative Rehabilitation • Protect Injury • Increase Pain Free Activity • Increase ROM • Increase Strength • Proprioception • Increase Flexibility • Sports Specific • CV Endurance
Post-Operative Protocols Return To Play Criteria • Full Strength • Full ROM • Functional Test • Physician Clearance • Protect Injury
Conclusion • Early Recognition • Determine Extent of Injury • Rule out Associated Injuries • Conservative Treatment (2-8 Weeks) • Surgical Intervention (4-8 Months) • Complications
References • Eric Nussbaum, Timothy M. Hosea, Shawn Sieler, Brian Incremona, Donald Kessler. Prospective Evaluation of Syndesmotic Ankle Sprains Without Diastasis. American Journal of Sports Medicine. 2001; 29:31-35. • David A. Porter. Evaluation and Treatment of Ankle Syndesmosis Injuries. [Editorial]. 2009; 58:575-581. • Cyrus M. Press, Asheesh Gupta, Mark R. Hutchinson Management of Ankle Syndesmosis Injuries in the Athlete. American Academy of Sports Medicine.2009; 8:228-233. • Marc L Wagener, Annechien Beumer, Bart A Swierstra. Chronic instability of the anterior tibiofibular syndesmosis of the ankle. Arthroscopic Findings and Results of Anatomical Reconstruction. Bio Med Central Musculoskeletal disorders 2011; 12:1-7. • Albert Alonso, Lynette Khoury, Roger Adams. Clinical Tests for Ankle Syndesmosis Injury: Journal of Sports and Physical Therapy. 1998; 27:276-284.