Download
1 / 78
890 likes | 1.6k Views
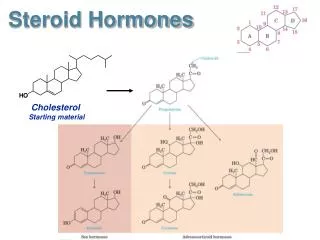
Steroid hormones. Assoc. Prof. Iv. Lambev E-mail: itlambev@mail.bg www.medpharm-sofia.eu. Corticosteroids. Δ 4-Androstendione. Testosterone. Pathways of corticosteroid biosynthesis. Glucocorticosteroid. Glucocorticosteroids diffuse into the cell, but access

E N D
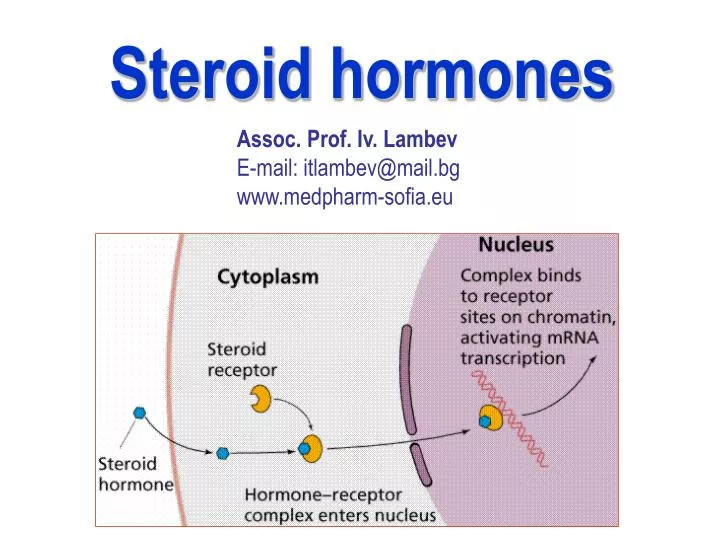
Steroid hormones Assoc. Prof. Iv. Lambev E-mail: itlambev@mail.bg www.medpharm-sofia.eu
Δ4-Androstendione Testosterone Pathways of corticosteroid biosynthesis
Glucocorticosteroid Glucocorticosteroidsdiffuse into the cell, but access to the receptor may be prevented, for example in kidney, by the enzyme 11-beta hydroxysteroid dehydrogenase, which converts active cortisol into inactive cortisone. When activated, the receptors translocate to the nucleus where they can upregulate gene transcription by action on specific DNA response elements.
ACTIONS OF HYDROCORTISONE (CORTISOL) The effects of hydrocortisone will be described as a basic glucocorticoid hormone. There is a distinction between replacement therapy (physiological effects) and the higher doses of pharmacotherapy. (1) On inorganic metabolism (mineralocorticoid effects): cortisol increasis retention of sodium by the renal tubule, and increasis potassium excretion in the urine.
(2) On organic metabolism (glucocorticoid effects): •Carbohydrate metabolism: gluconeogenesis is increased and peripheral glucose utilization (transport across cell membranes) may be decreased (insulin antagonism) so that hyperglycaemia and sometimes glycosuria result. Latent diabetes becomes overt. • Protein metabolism: anabolism (conversion of amino acids to protein) is decreased but catabolism continues unabated or even faster, so that there is a negative nitrogen balance with muscle wasting. Osteoporosis (reduction of bone protein matrix) occurs, growth slows in children, the skin atrophies and this, with increased capillary fragility, causes bruising and striae.
Healing of peptic ulcers or of wounds is delayed. • Fat deposition: this is increased on shoulders, face, and abdomen. • Inflammatory response is depressed; corticosteroids can be a source of danger in infections by limiting useful protective inflammation. Neutrophil and macrophage function are depressed, including the release of chemical mediators and the effects of these on capillaries. Glucocrticosterods have antiexudative and antiproliferative effects.
The anti-inflammatory actions of glucocorticoids are mediated by stimulation of synthesis of lipocortin, which inhibits pathways for production of eicosanoids (prostaglandins, leukotrienes, lipoxins), and platelet activating factor too. These mediators would normally contribute to increased vascular permeability and subsequent changes including oedema, leucocyte migration, fibrin deposition.
(-) (+)
Allergic responses are suppressed. The • antigen-antibody interaction is unaffected, but • its injurious inflammatory consequences do not • follow. • • Antibody production is reduced by heavy • doses. • •Lymphoid tissue is reduced (including leukaemic • lymphocytes). • • Renal excretion of urate is increased. • • Blood eosinophils are reduced in number. • • Euphoria or psychotic statesmay occur, • perhaps due to CNS electrolyte changes. • • Anti-vitamin D action.
Overview of the hypothalamic- pituitary- adrenal axis and the immune inflammatory network
• Reduction of hypercalcaemia chiefly where this is due to excessive absorption of calcium from the gut (sarcoidosis, vitamin D intoxication). • Urinary calcium excretion is increased and renal stones may form. • Growth reduction where new cells are being added (growth in children), but not where they are replacing cells as in adult tissues. • Suppression of hypothalamic/pituitary/adrenocor- tical feedback system (with delayed recovery) occurs with chronic use, so that abrupt withdrawal leaves the patient in a state of adrenocortical insufficiency.
The most used glucocorticoids Hydrocortisone Prednisolone Nonfluorinated prednisolones Fluorinated prednisolones Betamethasone Dexamethasone Triamcinolone Methylprednisolone
Structure and nomenclature of corticosteroid products and selected synthetic derivatives
Hydrocortisone (cortisol) is the principal naturally occurring steroid; it is taken orally; a soluble salt can be given i.v. for rapid effect in emergency (whether due to deficiency, allergy, or inflammatory disease). A suspension (Hydrocortisone Acetate) can be given intra-articularly. Prednisone is a prodrug, i.e. it is converted into prednisolone in the liver. Prednisolone is predominantly anti-inflammatory glucocorticoid, biologically active, and has little sodium-retaining activity; it is the standard choice for anti-inflammatory pharmacotherapy, orally or i.m.
Fluorinated glucocorticosteroids Triamcinolone has virtually no sodium retaining (mineralocorticoid) effect but has the disadvantage that muscle wasting may occasionally be severe and anorexia and mental depression may be more common at high dose. Dexamethasoneand Betamethasone are similar, powerful predominantly anti-inflammatory steroids. They are longer-acting than prednisolone and are used for therapeutic adrenocortical suppression.
Replacement glucocorticoid therapy • Acute adrenal insufficiency • Chronic adrenal insufficiency (Addison's disease) • Congenital adrenal hyperplasia • (adrenogenital syndrome) • Glucocorticoid pharmacotherapy • for non endocrine diseases • Steroids are powerful drugs. They may cause • dramatic improvement in many severe diseases • as well as produce equally severe adverse effects • if not properly used.
The use of steroids in non endocrine disease is • empirical and palliative, but may be life-saving. • The following general principles must be observed • (Tripathi, 2003): • Single dose (even excessive) is not harmful. • Short courses (even high dose) are not likely to • be harmful in the absence of contraindications. • Long-term use is potentially hazardous. • No abrupt withdrawal after a corticoid has been • given for more than 2 to 3 weeks: may • precipitate adrenal insufficiency.
1. Rheumatoid arthritis: corticoids are one of the last resort drugs. 2. Osteoarthritis. Intra-articular injection of steroid is rare, but may be used to control an acute exacer- bation. Repeated injections may cause joint destruction. 3. Rheumatic fever. Corticoids are used only in severe cases with myocarditis and CHF. 4. Collagen diseases: systemic lupus erythematosus, polyarteritis nodosa, dermatomyositis, nephrotic syndrome, glomerulonephritis. 5. Severe allergic reactions 6. Autoimmune diseases: autoimmune haemolytic anaemia, thrombocytopenia, active chronic hepatitis
7. Bronchial asthma 8. Eye diseases (as eye drops or ointment) in allergic conjunctivitis, iritis, iridocyclitis, keratitis. 9. Skin diseases: Topical glucocorticosteroids are used in many exematous skin diseases 10.Intestinal diseases: ulcerative colitis, Crohn’s disease, coeliac disease 11.Cerebral oedema due to tumours, tubercular meningitis, etc. 12.Malignancies: acute lymphatic leukemia, Hodgkin’s disease and other lymphomas 13.Organ transplantations and skin allograft 14.To test adrenal-pituitary axis, etc.
Adverse effects of Glucocorti- costeroids • Cushing’s syndrome • Osteoporosis • Tendency to hyperglycaemia • Negative nitrogen balance • Increased appetite • Increased susceptibility • to infections • Obesity, etc. Cushing’s syndrome
Contraindications • Peptic ulcer • Diabetes mellitus • Hypertension • Pregnancy (risk foetal defects) • Tuberculosis, mycoses, virosis • (including Herpes simplex keratitis), • and other infections • Osteoporosis • Psychosis • Epilepsy • Chronic heart failure • Renal failure
Mineralocorticoids Aldosterone (t1/2 20 min), the principal natural salt retaining hormone, has been used i.m. in acute adrenal insufficiency. After oral admini- stration, it is rapidly inactivated in the first pass through the liver but has no place in routine therapeutics, as fludrocortisone is as effective and is active orally.
Fludrocortisone has a very great sodium-retaining effect in relation to its anti-inflammatory action and only at high doses the nonelectrolyte effects need to be considered. It is used to replace aldosterone where the adrenal cortex is destroyed (Addison's disease). Fludrocortisone is also the drug of choice in most patients with autonomic neuropathy, in whom volume expansion is easier to achieve than a sustained increase in vasoconstrictor tone. Much higher doses of fludrocortisone (0.5 to 1 mg) are required when the cause of hypotension is a salt- losing syndrome of renal origin, e.g. following an episode of interstitial nephritis.
Sex (gonadal) hormones and antagonists • Androgens and antiandrogens • Estrogens and antiestrogens • Progestins and antiprogestins • Hormonal contraceptives
The biochemical • pathway in the • conversion • of cholesterol to: • androgens • (Dihydrotestosterone) • and • estrogens • (Estradiol)
Mechanism of action Steroid hormone receptors for gonadal and adrenocortical steroids are complex proteins inside the target cell. They penetrate into the cell and bind to a receptor. Complex steroid/receptor translocates into the cell nucleus, which is the principal site of action and where RNA/protein synthesis occurs. Compounds that occupy the receptor without causing translocation into the nucleus act as antagonists, e.g. spironolactone to aldosterone, cyproterone to androgens, clomiphene to estrogens.
Pharmacokinetics Steroid sex hormones are well absorbed through the skin. Most are subject to extensive hepatic metabolic inactivation (so much that oral administration is ineffective or requires very large doses). There is some enterohepatic recirculation, especially of estrogen, and this may be interrupted by severe diarrhoea to cause loss of efficacy. There are some nonsteroid analogues that are more slowly metabolized. Sustained-release (depot) preparations are used. The hormones in the blood extensively bind to sex-hormone-binding globulin. The plasma half live relates to the duration of cellular action, which is implied in the recommended dosage schedules.
Androgens Testosterone is the natural androgen secreted by the interstitial cells of the testis; it is necessary for normal spermatogenesis, for the development of the male secondary sex characteristics, and for the growth, at puberty, of the sexual apparatus. It is converted by hydroxylation to the active dihydrotestosterone. Protein anabolism especially in skeletal muscles is increased by androgens. Growth of bone is promoted, but the rate of closure of the epiphyses is also hastened, causing short stature in cases of precocious puberty or of androgen overdose in the course of treating hypogonadal children.
Pathway of synthesis of testosterone in the Leydig cells of the testes
Metabolism of testosterone to its major active and inactive metabolites
Androgen metabolism and actions. SHBG – sex hormone- binding globulin
Indications for androgen therapy Testicular failure.It may be primary or secondary (due to lack of pituitary gonadotrophins). In either case replacement with androgens is often necessary. Unfortunately, the sterility is not remedied, although loss of libido and of secondary sex charac- teristics can be greatly improved. If androgen is given to a boy with delayed puberty, a growth spurt and sexual development will occur. Androgens are now little used in metastatic breast cancer because of their virilising effects.
Androgen preparations Testosterone has extensive hepatic first-pass metabo- lism. It may be given orally or as i.m. depot injections. Mesterolone provides oral therapy. Antiandrogens (androgen antagonists) Estrogens and progestogens are physiological anta- gonists to androgens. But compounds which compete selectively for androgen receptors have been made. Cyproterone is a derivative of progesterone. It is used for reducing male hypersexuality and in prostatic cancer and severe female hirsutism.
A formulation of cyproterone plus ethinylestradiol (Diane®)is offered for the treatment of severe female hirsutism as well as for severe acne in women; this preparation acts as an oral contraceptive too. Cyproterone causes hepatomas in rats. It is unsuitable for male contraception. Flutamide and bicalutamide are nonsteroidal antian- drogens for use in conjunction with the gonadorelins (e.g. goserelin) in the treatment of prostatic cancer. Finasteride inhibits conversion of testosterone to dihydrotestosterone. It has antiandrogen activity in tissues where dihydrotestosterone is the principal androgen: this makes it a useful drug in the treatment of benign prostatic hyperplasia.
Spironolactone also has antiandrogen activity and may help hirsutism in women. Androgen secretion may be diminished by continued use of a gonadorelin (LH-RH) analogue. Ketoconazole (antifungal drug) inhibits androgen synthesis and may be used in prostatic cancer. Anabolic steroids Androgens are effective protein anabolic agents, but their clinical use for this purpose is limited by virilisa- tion of women. Attempts made to separate anabolic from androgenic action have been partially success- ful. All anabolic steroids have also androgenic effects.
Anabolic steroids (Nandrolone) may no longer be used in osteoporosis. They benefit some patients with aplastic anaemia.Hereditary angioedema may be prevented. Anabolic steroids can prevent the calcium and nitrogen loss in the urine that occurs in patients bedridden for a long time and they have therefore been used in the treatment of some severe fractures. The use of anabolic steroids in conditions of general wasting despite nutritional support may be justifiable in extreme debilitating disease, such as severe ulce- rative colitis, and after major surgery. In the later stages of malignant disease they may make the patient feel and look less wretched. Their general use as tonics is scandalous, as is their use in sport.
Estrogens Estrone and estradiol are both natural estrogens. Estrogens are responsible for the normal development of the female genital tract, of the breast, and of the female secondary sex character- istics. The pubertal growth spurt is less marked in females than in males, probably because estro- gens have less protein anabolic action than do androgens, although they are as effective in promoting closure of epiphyses.
Neuroendocrine control of gonadotrophin secretion in females
Blood estrogen concentrations must be above a critical level for the maintenance of both prolife- rative and (together with progesterone) secretory phases of the uterine endometrium. If the estro- gen level falls too low, uterine bleeding follows. Estrogens are necessary for the maintenance of normal pregnancy and for the accompanying breast hyperplasia. The vagina is more sensitive to estrogens than is the endometrium.
The menstrual cycle, showing plasma levels of pituitary and ovarian hormones and histologic changes
Hormonal relationships of the human menstrual cycle
Estrogen preparations Ethinylestradiol (t1/2 13 h) is a synthetic agent of first choice for contraceptive use; it is effective by mouth. Estradiol and estriol are orally active mixed natural estrogens. Their TTS can be effective and convenient for women who dislike oral therapy. Conjugated estrogens (Premarin®) are orally active mixed natural estrogens containing 50–65% estrone obtained from the urine of pregnant mares. Stilboestrol (diethylstilbestrol) is used in androgen dependent cancers (breast, prostate).
Replacement therapy in hypoestrogenaemia. This term refers to decreased estrogen production due to ovarian disease, or to hypothalamic/pituitary disease (hypogonadotropic hypogonadism). Treat- ment is by cyclic estrogen (conjugated estrogens or ethinylestradiol for 21 days) plus a progestogen, medroxyprogesterone for the last 10 to 14 days of estrogen treatment. An alternative treatment is the oral contraceptive. Unless the cause of the hypoovarian state is primary ovarian failure, treatment should be stopped after every third cycle to see if spontaneous menstruation will occur.
Postmenopausal hormone replacement therapy (HRT). It is the use of estrogen treatment to reverse or prevent problems due to the loss of ovarian hormone secretion after the menopause, whether physiological or induced. The tissues sensitive to estrogen include brain, bone, skin, cardiovascular and genitourinary system. The two aims of HRT are: (1) To reduce the everyday symptoms of estrogen loss: hot flushes, insomnia, lethargy and depression, vaginal dryness. (2) To prevent the long-term complications asso- ciated with estrogen deficiency: osteoporotic fractures and coronary heart disease.
All types of HRT (estrogen with or without progestogen) are effective in reducing the hot flushes experienced by more than 50% of postmenopausal women. The benefit is highest during the first year of treatment when 80% of women report a reduced likelihood of flushes. The other major value from HRT is the relief of vaginal dryness. Vaginal admini- stration (as a cream, ring, pessary, or tablet) is the most effective route for treatment of these symptoms. There are three types of regimen used for HRT: (1) Women without uterus take continuous estrogen alone.