Download

1 / 40
410 likes | 677 Views
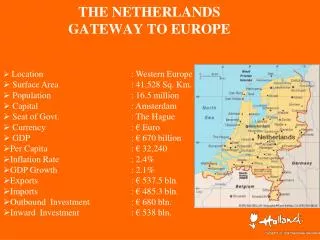
Assertive Outreach in The Netherlands and Europe. Copenhagen, November 2, 2012 Prof.dr. C.L. Mulder Chairman European Assertive Outreach Foundation. Contents. Assertive Outreach ACT and FACT in the Netherlands AO in Europe: quality of care for difficult to engage patients in large cities.

E N D
Assertive Outreach in The Netherlands and Europe Copenhagen, November 2, 2012 Prof.dr. C.L. Mulder Chairman European Assertive Outreach Foundation
Contents • Assertive Outreach • ACT and FACT in the Netherlands • AO in Europe: quality of care for difficult to engage patients in large cities
Assertive Outreach: a care delivery model • For patients with severe mental illness • Patients who need home-based care • Due to (periods of) lack of motivation • Inability to come to appointments
Motivation Paradox Classic Assumption Distress Motivation Problems Insight ↓ Motivation Paradox in SMI Motivation Negative experiences Problems Cognitive functioning ↓
Problem level and motivation for treatment in severely mentally ill ACT patients P<0.001 (Kortrijk et al. submitted)
Assertive Outreach • Effective ingredients (Burns et al. 2006) for association with reduction of hospitalisation • Smaller caseloads • Regular home visits • Responsibility for health and social care • Multidisciplinary team • Psychiatrist in the team
Assertive Community Treatment • Target group: • 20% most severely ill patients • Who do not seek treatment • Teamwork • Multidisciplinary • Implementing other EBP’s: IDDT, CBT, IPS • No brokerage • Small caseload (1:15) • Shared caseload • Outreach • No limits in duration of care
Flexible ACT: FACT • All patients with SMI • Multidisciplinary team • Providing EBP’s: CBT, IDDT, IPS, FPE • ACT model when needed • 200 patients • 10 fte • FACT Board
FACT: a Dutch version of ACT • For all patients with severe mental illness • Instead of ACT and ICM teams FACT • Increasing continuity of care • Flexible response (2 levels of intensity) • Regional teams » social inclusion • ‘Transmural’: linking hospital & community care
Six building blocks FACT
Ad1) FACT-board • Digital FACT BOARD • Shared Caseload • Shared knowledge / ideas • Discussed during daily meetings • Patients are put on the FACT board when: • Crisis situations • Intensive treatment is needed (major life events) • New situations (guidance in the working place) FACT NHN
Ad 2): EBP treatmentservice delivery model • Diagnosis and medication • Somatic screening • Psycho-education • Cognitive Behaviour Therapy (CBT) • Support of family and network • Individual Placement and Support (IPS) • Addiction: Integrated Dual Diagnosis Treatment (IDDT) and motivational interviewing FACT NHN
Ad 3) Recovery • Promoting: • Person-centered • Strengths- based • Collaborative care (shared decision making) • Empowering • Respect and Hope FACT NHN
Ad4) Binding to the mental health service network • Continuity of care between community and hospital • FACT team is responsible for treatment plan, also during admission • During admission, regular meeting client, family, CM FACT-team and team ward about goals of admission and length of stay
Ad 5) FACT and the community • Focussed on a specific region • Good opportunities for community care • Close contact with neighbourhood, G.P. and police • Accessible / Case-finding • Working with (individual) support systems on inclusion • Use naturally occurring resources • “Place then train principle”
Ad 6) • We will be there were the clients wants to be succesfull • OUTREACH!
Six building blocks FACT
Effectivity of (F)ACT: the evidence • American studies: ACT reduces hospitalisation days • European studies do not confirm these findings, except for less drop-out of care (Burns ea 2007) • European studies: more positive results in early psychosis patients (ACT+; Nordentoft et al. 2007))
Effectivity of (F)ACT: the evidence • FACT associated with more remission than ICM (Bak et al. 2009) • Association between high ACT model fidelity and more effect (Vught ea 2011) • Dismantling AO into FACT -> fewer admissions, less contacts (Firn et al. 2012) Conclusions: - Evidence for effectivity of (F)ACT in Europe limited - No RCT’s on effects of FACT! - Despite lack of evidence: (F)ACT teams in the Netherlands
Better model fidelity: more effect (Vugt et al. Can J Psychiatry 2011)
Center for Certification of ACT and FACT • Non profit foundation • Uses model fidelity scales: DACTS and FACTS • Certified and trained auditors • One day visit to the team using DACTS or FACTS • Cut off score levels used for certitication (DACTS: 3.7 and higher) • Certificate for model fidelity of ACT or FACT team • See: www.ccaf.nl
June 2012: > 200 (F)ACT-teams Blue: FACT Red: ACT Green: Specialized ACT
Benefits of certification • Better patient care • Team knows ACT or FACT model fidelity • Team knows what to improve • Managers know what the team is • Insurance companies who pay for care demand an ACT or FACT certificate
ACT and FACT for different populations • ACT and FACT hase been developed for different populations: • Firts episode psychosis • Youth • Elderly • Forensic • Addiction • Mentally Retarded • Model fidelity scales have also been developed
European Assertive Outreach FoundationAim: to improve outpatient care for (difficult to engage) SMI patients Second International Congress of AO June 26-28, 2012‘Improving Integration’
Study on AO in Europe Mulder et al. (submitted) • Experts in all European Countries were send a short questionnaire about AO in their country • Response rate: 22/27 (76% ) • (92% of all citizens)
Any care for difficult to engage patients? • Do difficult to engage patients with severe mental illness who are referred to the mental health system receive any form of assertive outreach in large cities? • 12 (69%): No • 9 (31%): Yes
Quality of Outpatient Care • How satisfied are you with the quality of outpatient care for patiens with severe mental illness in your country (Scale 0-10) • Mean: 5.2 • Min: 2 (Czech Republic) • Max: 8 (Denmark)
Quality of Outpatient Care for Difficult to Engage patients • How satisfied are you with the quality of outpatient care for Difficult to Engage patiens with severe mental illness in your country (Scale 0-10) • Mean: 3.2 • Min: 0 (Czech Republic) • Max: 8 (Denmark) • No association between gross national income and availability of AO
Conclusion AO in Europe • The quality of outpatient care for (difficult to engage) SMI patients in Europe is rated as inadequate • Increase in quality of care for SMI patients is needed in European countries • Introduction of FACT model in different countries? • Study: experts opinion on best practices for DEP in Europe
See you in Aviles, June 2013 Deadline abstracts for symposia, workshops, presentations, posters: december 1, 2012 http://www.eaofaviles2013.com/