Download
1 / 8
140 likes | 804 Views
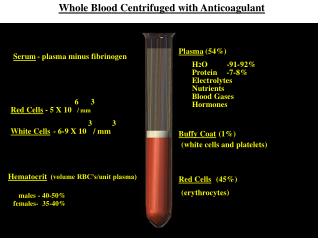
Whole Blood After transfusion with one unit of whole blood, 1.0g/dL hemoglobin indications for transfusion with whole blood are hemorrhagic shock with cogulation factor abnormalities. Packed Red Blood Cells

E N D
Whole Blood • After transfusion with one unit of whole blood, 1.0g/dL hemoglobin indications for transfusion with whole blood are hemorrhagic shock with cogulation factor abnormalities. Packed Red Blood Cells • General indications for use include the replacement of hemoglobin for oxygen carrying capacity in patients with reduced hemoglobin, such as patients with major trauma and bleeding, shock secondary to acute blood loss, intra operative blood loss > 750mL, and significant anemic states requiring intervention.
Massive Transfusion • Replacement of the patient’s blood volume over a 24 h period defines massive transfusion. Platelets • Transfusion of platelets is indicated for thrombocytopenia. • In a 70 kg adult, one platelet pack may be expected to increase the platelet count by 5,00 to 10,000/mm3 1h post transfusion. Granulocytes • Granulocyte transfusions are reserved for febiril neutropenic patients (<500 neutrophils/mm3) who have a good chance of bone marrow recovery and have bacterial or fungal infections unresponsive to ntibiotic therapy. Granulocyte transfusions may also be considered for septic, pancytopenic neonates with decreased bone marrow reserve.
Plasma Products • Plasma is indicated for patients with coagulation factor deficiency, hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, and antithrombin III deficiency. • Cryoprecipitate contains von Willebrand factor, factor VIII, fibrinogen, factor XIII, and fibronectin. It is used for therapy of von Willebrand’s disease, hemophilia A, factor XIII deficiency, and firbrinogen deficiency. It must be ABO matched . • Factor VIII concentrate is used for severe hemophilia A and in patients with significant factor VIII inhibitors. Factor IX concentrate is used to treat hemophilia B, deficiencies of factors II, VII, or X and factor VIII inhibitor.
Albumin and Plasma Protein Fraction • These products are derived from plasma, heat treated to prevent disease transmission, and indicated for patients who are hypovolemic and hypoproteinemic. • A 5% concentration of either solution has osmotic and oncotic properties equivalent to plasma.
Shock Definitions • Shock is the underprefusion of multiple organ systems. Initial Management • The mainstays of shock therapy are to 1. improve oxygen delivery (by raising hemoglobin concentration, cardiac output, or arterial saturation); 2. reduce oxygen consumption, and 3. identify and treat the precipitants of hypoperfusion.
Urgen resuscitation of the Patient with Shock; Intravenous Volume and Vasoactive Drug Therapy 1. Hemorrhagic Shock including Truma, Raptured Aneurysms • Elevate legs, MAST • Access/infuse emergency blood Group/Match /Administer warmed blood/ Components • >3L/20 min warmed saline equal volumes of colloid or substitutes (albumin, dextran, hetastarch) • Continue aggressive volume infusion until blood pressure normal. • Consider early surgical hemostasis • Awaiting adequate volume repletion, institute multipurpose agent (dopamine or epinephrine) and increase does from 1 towards 10 (g/kg/min for dopamine; g/min for epinephrine) as needed to maintain blood pressure. • If higher doses are needed, add norepinephrine (2-20 g/min ). • Discontinue these drugs as urgently as volume repletion and hemostasis allow (see Second column).
2. Nonhemorrhagic Hypovolemia including septic shock • Elevate legs • L/20 min warmed saline • Group/match packed RBCs and plasma re dilutional anemia • Continue aggressive volume infusion until blood pressure normal or heart “too full” • Detect and treat tamponade with pericardiocentesis, thoracostomy, peritoneal drainage, or reduced PEEP • Avoid vasoactive drug until heart “too full” • Except dopamine (2-5 g/kg/min) for renal perfusion early. • Nitroglycerin and nitroprusside are contraindicated. • Vasoconstrictors delay adequate volume repletion (see left column). • In right heart overload with shock norepinephrine (2-20 g/min) may help by maintaining RV perfusion; in septic shock, vasoconstrictors may replacement provides inadequate perfusion pressure (see text ).
3. Cardiogenic Shock due to Myocardial Ischemia • When heart is “too full” decreasing blood volume (rotating tourniquets, phlebotomy, nitroglycerin, morphine, diuretics). • If the heart is not “too full” or blood pressure decreasing with above interventions, NS 250ml/20 min • Repeat if blood pressure increasing until heart too full. • Dobutamin (5-15 g/kg/min) to enhance contractility wihout excess tachycardia, arrhythmia, or vasconstriction; higher doses dilate skeletal vascular bed. • Dopamine (g/kg/min) to preserve renal cortical blood flow; at higher dose (4-12 g/kg/min) increases heart rate, contractility, venous tone, and preload, like epinephrine. • Nitroglycerin (5-250 g/min) for venodilation with minimal arterial dilation except for the coronary circulation. • Sodium nitroprusside (0.1-10 g/kg/min)for arterial dilation to reduce afterload and allow greater ejection from a depressed left ventricle or regurgitant aortic/mitral valve