Download
1 / 15
370 likes | 2.06k Views
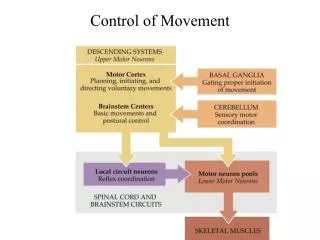
Brain Control of Movement . Motor Control Hierarchy. High level – plans and executes strategy Association areas of cortex Basal ganglia gives the “go” signal Middle level – develops tactics Motor cortex Cerebellum Low level – executes movement Brain stem, spinal cord.

E N D
Motor Control Hierarchy • High level – plans and executes strategy • Association areas of cortex • Basal ganglia gives the “go” signal • Middle level – develops tactics • Motor cortex • Cerebellum • Low level – executes movement • Brain stem, spinal cord
Two Pathways to the Brain • Two pathways: • Lateral pathway • Ventromedial pathway • Lateral pathways control fractionated movement of distal muscles, especially flexors, under direct cortical control: • Corticospinal – new, originates in motor cortex • Rubrospinal – old, originates in red nucleus of midbrain
Ventromedial Pathways • Four pathways control proximal & axial muscles. • Vestibulospinal – maintains stability of head and turns it, maintains upright posture & balance • Input from labyrinth of inner ear • Tectospinal – orients eyes (fovea) on image • Receives input from superior colliculus • Pontine – resists gravity and maintains posture • Medullary – liberates muscles from anti-gravity control
Voluntary Movement • Involves almost all of the cortex. • Goal-directed movement depends on: • Knowing where the body is in space. • Knowing where it wants to go. • Selection of a plan to get it there. • Once a plan is devised, it must be kept in memory until it can be executed. • Instructions to implement the plan must be issued. • These functions are localized to different areas.
Parts of the Motor System • Premotor areas (PMA, SMA) – plan the motor activity • Primary motor cortex (M1) – initiates motor activity: • Basal ganglia loop (near thalamus) gives the “go” signal • Cerebellar loop – tells the motor cortex how to carry out the planned activity • Controls direction, timing and force by activating populations of motor neurons in learned programs.
Planning Movement • Goal directed movement involves many cortical areas that communicate with Area 6 in Frontal lobe. • Area 6 has two parts: • PMA (premotor area) • SMA (supplemental motor area) – lesions produce apraxia (impaired complex acts) • Area 6 plans an action and stays active until it is executed (“go” signal).
The “Go” Signal • Area 6 receives a “Go” signal from the thalamus (VLo). • Input to the thalamus comes from the basal ganglia deep in subcortical areas. • A circuit through the basal ganglia inhibits excitation of the SMA by VL. • Inhibition is released by the substantia nigra, permitting VL to send a “go” signal to the SMA.
Disorders of Movement • Hypokinesia – a lack of movement caused by increased inhibition of the thalamus by the basal ganglia. • Hyperkinesia – too much movement caused by decreased basal ganglia input, removing inhibition of the thalamus. • Bradykinesia – slowness of movement. • Akinesia – difficulty initiating movement.
Parkinson’s Disease • Caused by degeneration of the substantia nigra and depletion of dopamine. • Impairs the “go” signal circuit to VLo & SMA. • Symptoms are bradykinesia, akinesia, increased muscle tone (rigidity), tremors of hands and jaw, especially at rest. • Treated by the drug L-Dopa, the precursor to dopamine.
Huntington’s Disease • Hereditary, progressive, lethal syndrome caused by loss of neurons in the basal ganglia, cortex, and elsewhere. • Symptoms are hyperkinesia, dyskinesia (abnormal movement), dementia (impaired cognition), and personality disorders. • Chorea – uncontrolled and purposeless movement with rapid, irregular flow and flicking motions.
Ballism • Caused by damage or lesions to the basal ganglia, usually resulting from stroke. • Loss of excitation of the global pallidus (normally inhibiting VLo) results in too much excitation of SMA. • Symptoms are violent, flinging movements of the extremities.
Coding the Direction of Movement • Motor cortex (M1) neurons fire at different rates depending on the desired direction. • Firing rates are averaged across populations of M1 neurons. • When contributing neurons are inhibited, resultant direction changes. • Cerebellum controls sequence.
Cerebellum • Creates a detailed sequence of precisely timed muscle contractions needed to execute movement. • Ataxia – uncoordinated, inaccurate movement. • Dyssynergia – decomposition of synergistic muscle movements. • Dysmetric – imprecise movement, overshooting or undershooting target. • Alcohol impairs cerebellar functioning.
Cerebellar Motor Loop • Cerebellum supplies input to the motor cortex via the pons (pontine nuclei) and area VLc of the thalamus. • Feedback from the sensory cortex guides activity of the cerebellum to create and store learned programs of movement. • Cerebellum compares what was intended with what happened, then modifies circuits to compensate.