Download
1 / 78
780 likes | 809 Views
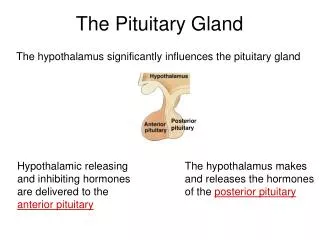
The Pathology of Pituitary. Doç. Dr. A. Işın DOĞAN-EKİCİ. Anatomy. The anterior lobe develops from an evagination of Rathke’s pouch (from the primitive oropharynx). The pituitary gland is located in the Sella Turcica in the base of the skull.

E N D
The Pathology of Pituitary Doç. Dr. A. Işın DOĞAN-EKİCİ
Anatomy • The anterior lobe develops from an evagination of Rathke’s pouch (from the primitive oropharynx). • The pituitary gland is located in the Sella Turcica in the base of the skull. • The anterior pituitary is one of the most vascularized tissues in the body, due to its portal system. • Secretion occurs in a 24 hr circadian rhythm . • The functions of the pituitary gland are controlled by factors produced in the hypothalamus.
Anatomy The anterior lobe develops from an evagination of Rathke’s pouch (from the primitive oropharynx).
The pituitary gland is located in the Sella Turcica in the base of the skull.
The anterior pituitary is one of the most vascularized tissues in the body, due to its portal system.
Topography of Hormone producing cells in the pituitary • The anterior hypophisis can be subdivided into four parts: • Two lateral wings................produce growth hormone • Medial portion: • a)Medial posterior.................ACTH • b)Medial Anterior..................TSH
Cell types Anterior Pituitary • Classification by H&E Staining: • Eosinophilic Cells: • Somatotropes (growth hormone), • Lactotropes (Prolactin) • Basophilic Cells: • Gonadotropes (FSH,LH) • Thyrotropes (TSH) • Corticotropes (ACTH) • Melanotropes (MSH) • Chromophob cells: • No activity/Prolactin • Crook’s hyaline -basophilic change in anterior pituitary cells in Cushing’s Syndrome
Diseases of Pituitary • Hormone Production imbalances: • Impaired Synthesis or release • Abnormal target tissue interraction • Abnormal target tissue response • Mass Lesions: • Non-functioning • Functioning
Clinical Classification Hyperpituitarism Hypopituitarism (Simmonds's disease) DISEASES of the PITUITARY GLAND
Multiple endocrine neoplasia syndromes • MEN 1 Syndrome (Werner's Syndrome) • MEN 2a Syndrome (Sipple Syndrome) • MEN 2b Syndrome (William Syndrome) • Common autosomal dominant conditions which predispose patients to certain endocrine tumors. • Pre-natal diagnosis is available for these tumor-gene syndromes.
MEN 2a Syndrome (Sipple Syndrome) MEN 2b Syndrome (William Syndrome)
Hyperpituitarism • Too much of one (or may be two or more) of the hormones from the adenohypophysis. • This may be due either to: • (1) autonomous over-production (tumors of the adenohypophysis: adenoma/carcinoma; ~ 15% of all primary intracranial tumors),or • (2) excess production of hypophyseal stimulating factors, or • (3) Underproduction of inhibiting factors, or • (4) Loss of inhibition following destruction of other endocrine glands.
Tumors ANTERIOR LOBE ADENOMAS • Pituitary adenomas constitute 10% of all diagnosed primary intracranial tumors. • They can occur at any age, • No great sex predominance. • They are more common in patients with autosomal dominant multiple endocrine neoplasia (MEN) 1 (Werner's)syndrome.
Pituitary adenomas typically present as one or more of the following: • (1) Endocrine problems (both from hormones produced by the tumor itself and from damage to the rest of the adenohypophysis and/or the neurohypophysis) • (2) Visual problems (from an expanding mass impinging on the optic chiasm, i.e., bitemporal hemianopsia) • (3) Enlarged sella turcica on skull x-rays (due to expanding masses; large pituitary adenomas eventually erode the sella, clinoid processes, diaphragma sellae, optic nerves and chiasm, and even the cavernous sinuses, nasal sinuses, or brain. • (4) Increased intracranial pressure (i.e., headache, nausea and vomiting).
(5) Hemorrhage (Hemorrhage into a large pituitary adenoma can produce pituitary apoplexy, which can simulate a berry aneurysm rupture). • (6) Infarct (Large tumors may also infarct themselves, leading to remission or destruction of the remaining normal gland as well).
Microscopy: Pituitary adenomas are typical endocrine adenomas, i.e. they are composed of cuboidal cells, with round nuclei and a good blood supply. • Acidophilic adenomas (eosinophilic adenomas) typically make growth hormone and/or prolactin. • Basophilic adenomas typically make ACTH; less often, they make TSH or the gonadotropins. • Chromophobe adenomas nothing (null cell adenoma) or may make prolactin.
Pituitary Adenomas Immunocytochemical Classification
Pituitary Adenomas Causing Growth Hormone Excess • somatotroph adenoma • mammosomatotroph adenoma Pituitary Adenomas Causing Prolactin Excess • lactotroph adenoma • psammoma bodies • endocrine amyloid • acidophilic stem cell adenoma
Lactotroph adenomapsammoma bodies a pituitary stone:extensive form of psammoma bodies
Lactotroph adenomas produce endocrine amyloid that stains with Congo red
Lactotroph adenoma: Intense diffuse positivity for PRL throughout the cell cytoplasm
Acidophilic stem cell adenoma:The acidophilia is attributable to mitochondrial accumulation, considered to be a form of oncocytic change
Pituitary Adenomas Causing Thyrotropin Excess (TSH) Pituitary Adenomas Causing ACTH Excess (ACTH) • corticotroph adenoma • crook's cell adenoma Pituitary Adenomas Causing Gonadotropin Excess (FSH)
Clinically Nonfunctioning PituitaryAdenomas • silent somatotroph adenomas • silent thyrotroph adenomas • silent lactotroph adenomas • silent corticotroph adenomas • silent gonadotroph adenomas • poorly differentiated adenomas Plurihormonal Adenomas Pituitary Carcinoma
Prolactinoma (30%) • Men: impotence, loss of libido • Women: amenorrhea, loss of libido, infertility • Both: Obesity, Galactorrhea • Growth hormone adenoma (20%) • Children: gigantism • Adults: acromegaly • Corticotroph cell adenoma (ACTH;15%) • Cushing's disease
Hyperprolactinemia • (1) Functioning Prolactinomas • (2) Hypothalamic tumors (Stalk effect)* • craniopharyngiomas, • gliomas, • hypothalamic germinomas *Stalk effect: This may be seen with any disease within or near the pituitary gland and stalk that interferes with the delivery of dopamine (a neurotransmitter) from the hypothalamus to the prolactin secreting cells of the pituitary. Therefore, other types of pituitary adenomas, craniopharyngiomas or other tumors or masses may cause modest elevations in prolactin.
(3)Medications • neuroleptics, • antidepressants • alfa-methyldopa. • (4) Other causes of Hyperprolactinemia • pregnancy or in the post-partum period • stress (discomfort, exercise, low blood sugar) • low thyroid function (hypothyroidism) • kidney failure • liver failure.
Gigantism &Acromegaly • Overproduction of growth hormone causes excessive growth. • In children: gigantism • In adults: acromegaly. Gigantisim • hormone production starts before the growth plates have closed • the long bones grow enormously. • great stature, and the arms and legs lengthen • hypogonadism (delayed puberty, genitals may not develop fully).
Acromegalia • prognathism • huge brows • huge tongue • huge hands (with "spade fingers") • develops a deep guttural voice • oily skin (extra sebaceous glands), odor • joint deformities (degenerative arthritis) • barrel chest • secondary diabetes • sleep apnea • cardiomegaly • irregular menstrual cycles and galactorrhea.
Cushing's disease • Excessive cortisol levels in the blood • Etiology • tumors of the pituitary gland (~70%), • tumor/hyperplasia* of the adrenal glands • ectopic ACTH producing tumors (lung: small cell ca) • Production of ACTH by a pituitary tumor • ACTH-oma: usually smallmicroadenomas • Nelson’s syndrome *Most cases of "idiopathic adrenal hyperplasia" are due to ACTH-omas.