Download
1 / 16
170 likes | 190 Views
Hypertension & diabetes: new guidelines. Janice Douglas, MD Case Western University Cleveland, OH George L Bakris, MD Director of the Hypertension/Clinical Research Center at Rush Medical College Chicago, IL. Hypertension and diabetes. What we know.

E N D
Hypertension & diabetes: new guidelines Janice Douglas, MD Case Western University Cleveland, OH George L Bakris, MD Director of the Hypertension/Clinical Research Center at Rush Medical College Chicago, IL
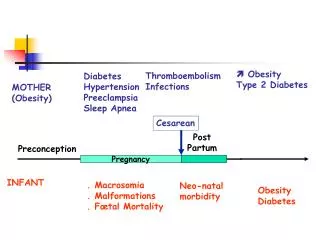
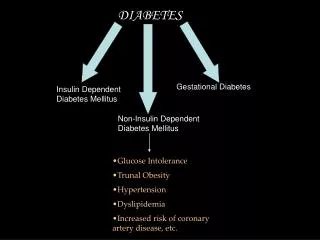
Hypertension and diabetes What we know More than 11 million Americans have both diabetes and hypertension as comorbid diseases. Increases in: urinary albumin excretion hyperuricemia dyslipidemias left ventricular hypertrophy Diabetes is the leading cause of end-stage renal disease in the general population.
Hypertension and diabetes Basis of NKF guidelines Based on JNC VI guidelines: BP <130/85 Trials suggest linear relationship between lower BP and lower cardiovascular risk (HOT, UKPDS) NKF guidelines: <130/80 Bakris GL, et al. Am J Kidney Dis 2000;36(3):646-661
Hypertension and diabetes Achieving the goal If BP >145/90, 2 or more medications needed to reach goal ACE inhibitor/diuretic is ideal starting combination Titrate ACE to max, keep diuretic low dose Watch for pulse rates higher than 84
Hypertension and diabetes Medication An average of 3.2 different antihypertensives are needed to reach this goal. The worse the renal function, the more medications you need (4 or 5).
Hypertension and diabetes Importance of BP management Tight BP control stronger than tight glucose control for lowering risk of: stroke death by diabetes any diabetic endpoint microvascular complications (UKPDS) BMJ 1998 Sep 12;317(7160):703-13
Hypertension and diabetes “I think it is critically important that the goal blood pressure be achieved [and that] people not become wimpy in terms of their anti-hypertensive medication doses.” George L Bakris, MD Director of the Hypertension/Clinical Research Center at Rush Medical College Chicago, IL
Hypertension and diabetes Reaching the goal General hypertensive population reaching JNC VI goal of <130/85: <30% Patients with diabetes and hypertension reaching JNC VI goal of <130/85: 11% Patients with diabetes and hypertension reaching NKF goal of <130/80: ????
Hypertension and diabetes Critical issues • Team approach (physician, nurse clinician, nurse, dietician) • Timing of medication (once daily dosing, fixed-dose combinations) • Education (What is the goal and why? Enlist the patient as active participant.)
Hypertension and diabetes Physician outreach 1) CME programs (classes of drugs and BP control) 2) Recertification (test them on recertification exam)
Hypertension and diabetes Fear of a J-shaped curve Fear is preventing the achievement of these goals: 1) No study with aggressive blood pressure control shows a J-shaped curve in cardiovascular events. 2) Fear of renal dysfunction is preventing adequate use of ACE inhibitors.
Hypertension and diabetes ACE-inhibitors and CCBs In combination, these agents produce an additive reduction in blood pressure. There is a reduction in the incidence of edema and proteinuria. Adding a diuretic gives “more bang for your buck”.
Hypertension and diabetes Socioeconomic factors How medical information is disseminated and how it is put forth have a huge impact on how the patient accepts the information. Physicians must become aware that cultural factors impact treatment.
Hypertension and diabetes Specific barriers Hispanic community barriers: Language barrier Males reluctant to come in Preconceived notions about medication Attempted solutions: Translators from the same culture Build confidence and trust “Shortcut approach” doesn’t work
Hypertension and diabetes Lifestyle Diet and exercise go hand in hand with other approaches. DASH study reduced BP in hypertensive subjects: Systolic (mm Hg) -11.5 + 1.3 Diastolic (mm Hg) -5.7 + 0.9 Svetkey LP, et al. J Am Diet Assoc 1999; 99(s8): s96-104
Hypertension and diabetes Pocket guide Pocket-sized version of treatment algorithm Executive summary of the guidelines National Kidney Foundation 1.800.622.9010