Download

1 / 27
270 likes | 280 Views
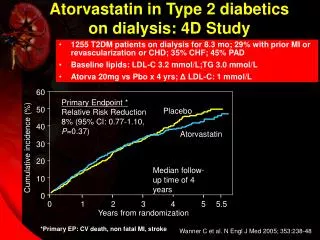
Atorvastatin: Effective Therapy for a Broad Range of Dyslipidemias. For individuals with:. Trial of dietary therapy and counselling:. Initiate drug therapy if LDL-C remains:. LDL-C Goal:. No CHD and <2 CHD risk factors. 6-12 months. > 190 mg/dL > 4.9 mmol/L. <160 mg/dL <4.1 mmol/L.

E N D
Atorvastatin: Effective Therapy fora Broad Range of Dyslipidemias
For individualswith: Trial of dietarytherapy andcounselling: Initiate drugtherapy ifLDL-C remains: LDL-CGoal: No CHD and<2 CHD riskfactors 6-12months >190 mg/dL>4.9 mmol/L <160 mg/dL<4.1 mmol/L No CHD and>2 CHD riskfactors 3-6months >160 mg/dL>4.1 mmol/L <130 mg/dL<3.4 mmol/L EstablishedCHD 6-12 weeks >130 mg/dL>3.4 mmol/L <100 mg/dL<2.6 mmol/L NCEP Guidelines for LDL Cholesterol NCEP. Circulation. 1994;89:1329-1445.
FraminghamHeart Study MRFIT Screenees Major Studies Showing Relationship Between Cholesterol Levels and CHD Risk (Pre-Statin Studies) Study type Size of cohort Conclusions Epidemiologic 5127 (original) 1% in cholesterol =2% in CHD risk Observational 361,662 Continuous, gradedassociation betweencholesterol level and CHDrisk starting at 180 mg/dL Castelli WP. Can J Cardiol. 1988;4(suppl A):5A-10A. Neaton JD, Wentworth D. Arch Intern Med. 1992;152:56-64.
LRC-CPPT Helsinki Heart Study Study type Treatment Effect on lipids Impact on CHD risk Prospectivecomparative Cholestyramine TC 9%LDL-C 13% 19% in risk of nonfatal MI or fatal CHD Prospectivecomparative Gemfibrozil TC 9%LDL-C 8%HDL-C 10%TG 34% 34% in risk of fatal and nonfatal MI or cardiac death Major Studies Showing a Beneficial Effect of Lipid-Lowering Therapy on CHD Risk (Pre-Statin Studies) Lipid Research Clinics Program. JAMA. 1984;251:351-364. Frick MH et al. N Engl J Med. 1987;317:1237-1245.
4S Results • 30% in risk of total (all-cause) mortality* • 34% in risk of major coronary events† • 42% in risk of definite and suspected CHD death • Changes in lipids: • 25% in Total-C — 8% in HDL-C • 35% in LDL-C • 10% in TG *P=0.0003; †P<0.00001. Scandinavian Simvastatin Survival Study Group. Lancet. 1994;344:1383-1389.
WOSCOPS Results • 31% in risk of nonfatal MI or CHD death* • 33% in risk of definite and suspected CHD death† • 22% in risk of all-cause mortality‡ • Changes in lipids: • 20% in Total-C — 5% in HDL-C • 26% in LDL-C • 12% in TG *P<0.001; †P=0.042; ‡P=0.051. Shepherd J et al. N Engl J Med. 1995;333:1301-1307.
CARE: Preliminary Results • 24% in risk of fatal CHD or nonfatal MI* • 25% in risk of fatal or nonfatal MI† • 27% in need for coronary revascularization‡ • Changes in lipids: • 20% in Total-C — 5% in HDL-C • 28% in LDL-C • 14% in TG *P=0.002; †P=0.007; ‡P=0.0001. Braunwald E, Pfeffer MA, Sacks FM. Presented at the 45th ACC; March 26, 1996; Orlando Fla.
Benefits of Hypolipidemic Treatment 0% 20% LRC-CPPT % Reduction inRisk ofCardiac End Points WOSCOPS 40% 4S ? 70% 10 13 26 35 60 % LDL-C Reduction
CH3 CH3 OH OH CH O O • Ca – 2+ CH2 CH CH NHC O CH2 CH2 CH2 N F 2 Chemical Structure of Atorvastatin
Cholesterol Biosynthesis Pathway HMG-CoA reductase Squalene synthase Dolichol Acetyl CoA HMG- CoA Farnesyl pyrophosphate Mevalonate Squalene Cholesterol Ras protein Farnesyl- transferase E,E,E-Geranylgeranyl pyrophosphate Farnesylated proteins Geranylgeranylated proteins Ubiquinones
Mechanism of Action of Atorvastatin Conclusions Based on Animal Studies • EH rabbits: LDL production • EHT rats: VLDL production • Guinea pigs: LDL production Atorvastatin inhibits hepatic production of major apo B-containing lipoproteins as shown in these animal models – Auerbach BJ et al. Atherosclerosis. 1995;115:173-180.Krause BR. Newton RS. Atherosclerosis. 1995;117:237-244.
6 N=154 Phase I No. of Studies 6 N=380 Phase II N=3150 Phase III 25 0 500 1000 1500 2000 2500 3000 No. of Subjects Atorvastatin Clinical Development
10 0 -10 -20 -30 -40 -50 -60 -70 Atorvastatin Dose-Response Study Mean Percent Change in LDL-C at 6 Weeks 7.6 % 41 44 50 * * * 61 * Placebo 10 mg 20 mg 40 mg 80 mg *P<0.05 vs placebo. Nawrocki JW et al. Arterioscler Thromb Vasc Biol. 1995;15:678-682.
Atorvastatin in Hypertriglyceridemia Design and Baseline Lipids • 56 hypertriglyceridemic patients, 26-74 y/o • 4-week, randomized, double-blind, placebo-controlled, parallel • Atorvastatin 5, 20, 80 mg • Mean baseline LDL-C: 119 mg/dL (3.1 mmol/L) • Mean baseline TG: 603 mg/dL (6.8 mmol/L) • Mean baseline HDL-C: 32 mg/dL (0.8 mmol/L) Bakker-Arkema RG et al. JAMA. 1996;275:128-133, and data on file, Parke-Davis (981-38).
Atorvastatin in Hypertriglyceridemia Mean Percent Change in Lipids at 4 Weeks 20 * 10 13 12 9 4 0 1 9 -10 Placebo Atorvastatin 5 mg Atorvastatin 20 mg Atorvastatin 80 mg 17 % * -20 26 32 -30 33 * *† 41 -40 46 *† * -50 TG LDL-C HDL-C *P<0.05 vs placebo; †P<0.05 vs 5-mg dose. Bakker-Arkema RG et al. JAMA. 1996;275:128-133.
10 0 -10 % -20 -30 -40 Atorvastatin vs Lovastatin Mean Percent Change in Lipids at 16 Weeks * * * * * 7 7 * 1 1 4 4 1 3 5 6 * * Placebo Atorvastatin 10 mg Lovastatin 20 mg 17 17 19 20 * * 27 27 28 * 36 Total-C LDL-C Apo B VLDL-C TG HDL-C *PŠ0.05 vs atorvastatin. Bakker-Arkema RG et al. Atherosclerosis. 1996, and data on file, Parke-Davis (981-08).
10 8 6 0 9 -10 16 17 17 % -20 24 25 27 -30 35 -40 Atorvastatin vs Pravastatin Mean Percent Change in Lipids at 16 Weeks Atorvastatin 10 mg Pravastatin 20 mg * * * * Total-C LDL-C Apo B TG HDL-C *PŠ0.05. Egros F et al. Atherosclerosis. 1996, and data on file, Parke-Davis (981-09).
10 0 -10 % -20 -30 -40 Atorvastatin vs Simvastatin Mean Percent Change in Lipids at 16 Weeks 7 7 Atorvastatin 10 mg Simvastatin 10 mg 15 23 -23 24 * 29 30 30 34 * 37 * * Total-C LDL-C Apo B TG HDL-C *PŠ0.05. Bracs P et al. Atherosclerosis. 1996, and data on file, Parke-Davis (981-37).
0 -10 -20 -30 -40 -50 -60 -70 Mean Percent Reduction in LDL-C in Fredrickson Type II Patients in Five Clinical Trials 981-13 981-04 981-43 981-04 981-07 981-04 981-44 981-04 % Reduction in LDL-C 35 39 41 45 44 50 57 61 10 mg 20 mg 40 mg 80 mg Atorvastatin Dose Black DM. Intl Congress Series No. 1066. 1995:307-310, and data on file, Parke-Davis.
0 Pravastatin -20 -30 %Changein LDL-C Fluvastatin -40 Lovastatin Simvastatin -50 -60 Atorvastatin -70 0 10 20 40 60 80 Dose (mg/d) Atorvastatin: LDL-C Reduction vs Other Statins Adapted from Black DM. Intl Congress Series No. 1066. 1995:307-310.
40 20 0 -20 -40 -60 Atorvastatin in Heterozygous FH Patients Percent Change in Lipids at 6 Weeks * 25 † * * % 34 45 57 Total-C LDL-C TG HDL-C *P<0.001; †P<0.01. Marais AD et al. Atherosclerosis. 1994;109:316.
0 -5 -10 -15 -20 -25 -30 -35 Atorvastatin Efficacy in Homozygous FH Receptor Negative (N=2) Baseline LDL-C: 498 mg/dL (12.9 mmol/L) Receptor Defective (N=6) Baseline LDL-C: 521 mg/dL(13.5 mmol/L) 3 Percent Reduction in LDL-C 17 22 Atorvastatin Simvastatin 35 Marais AD et al. 12th DALM Symposium; Nov 7-10, 1995; Houston, Tex.
30 20 10 0 % -10 -20 -30 -40 -50 Atorvastatin in Postmenopausal Women Mean Percent Change in Lipids at 12 Weeks * 16 11 4 9 2 1 7 5 7 9 3 Placebo Atorvastatin 10 mg Placebo + Estradiol 1 mg Atorvastatin 10 mg+ Estradiol 1 mg * 30 31 * 43 46 * Total-C TG LDL-C HDL-C *P<0.05 vs estradiol. Heinonen T et al. Atherosclerosis. 1996.
10 8 8 0 % Change -10 15 Atorvastatin Simvastatin -20 24 27 30 30 -30 * 39 -40 * Total-C LDL-C TG HDL-C Atorvastatin vs Simvastatin in NIDDM Effects on Lipids at 4 Weeks *P<0.01. Best JD et al. Atherosclerosis. 1994;109:312, and data on file, Parke-Davis (981-13).
Atorvastatin Medical Therapy vs Recanalization (AVERT) • Primary: incidence rate of ischemic events, time to ischemic event • Secondary: all-cause mortality, lipid profile, angina classification, QOL • Economic assessment of outcomes Patient Population (N=320): RecanalizationProcedure Usual Care • LDL-C 130 mg/dL (3.4 mmol/L) • TG Š400 mg/dL (4.5 mmol/L) • Asymptomatic tomoderately symptomatic • 1 lesion 50%-90%stenosis + Titrate to LDL-C Š100 mg/dL Š2.6 mmol/L Atorvastatin 80 mg/d 0 18 Month Efficacy Parameters McCormick L et al. Atherosclerosis. 1996, and data on file, Parke-Davis (981-68).
Atorvastatin Safety Summary • Administered to >3000 participants in clinical trials worldwide • 3 serious adverse events possibly attributable to atorvastatin have been reported • ALT elevations >3x ULN: <1% overall • No incidence of myopathy • <2% withdrawn due to associated adverse events Data on file, Parke-Davis.
Atorvastatin: Conclusions • Atorvastatin has a positive dose-response relationship over the range of 10-80 mg • LDL-C reductions from 40% to 60% • Effective in the broadest range of patients, including hypercholesterolemia, mixed dyslipidemia, hypertriglyceridemia, and homozygous FH • Safe and well tolerated in studies up to 2 years

![ARMYDA-CIN Trial [ Atorvastatin for Reduction of Myocardial Damage during Angioplasty–Contrast-Induced Nephropathy ]](https://cdn0.slideserve.com/625136/slide1-dt.jpg)