Download
1 / 42
430 likes | 440 Views
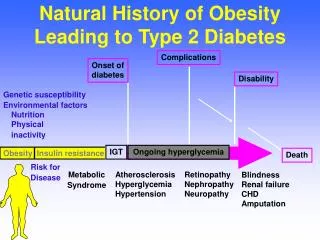
Update from Recent Trials Professor Kausik Ray Professor of Cardiovascular Disease Prevention BSc (hons), MBChB, MD, Mphil (Cantab), FRCP, FACC, FESC, FAHA. The dyslipidemia of intra-abdominal obesity and Type 2 diabetes. VLDL. LDL. HDL. Normal. Insulin resistance. VLDL triglycerides

E N D
Update from Recent TrialsProfessor Kausik RayProfessor of Cardiovascular Disease PreventionBSc (hons), MBChB, MD, Mphil (Cantab), FRCP, FACC, FESC, FAHA
The dyslipidemia of intra-abdominal obesity and Type 2 diabetes VLDL LDL HDL Normal Insulin resistance VLDL triglycerides VLDL apo B HDL cholesterol Particle number Particle size (small,dense) LDL apo B Particle number Particle size (small,dense)
Atherogenic Particles • MEASUREMENTS: Apolipoprotein B or Non-HDL-C VLDL VLDLR IDL LDL Small,denseLDL TG-rich lipoproteins
HDL can be categorised by shape, size & composition Particle shape Apolipoprotein composition eg A-I HDL A-I/A-II HDL E-containing HDL Discoidal Spherical Particle size Pre-beta HDL HDL2b HDL2a HDL3a HDL3b HDL3c Adapted from Barter PJ. Atheroscler Suppl. 2002;3:39–47.
Why Does HDL Protect?Beyond Cholesterol Transport endothelial repair anti-apoptotic protection against oxidation anti-inflammatory modulation of endothelial function antithrombotic HDL cholesterylester donor Cholesterol Transport
What is the best measure of atherogenic risk LDL-C, Non-HDL-C or apo B
Associations of major lipids and apoproteins with CHD HR 95% Cl 1.38 1.59 1.58 0.77 0.78 0.96 1.09 - 1.73 1.36 – 1.85 1.36 – 1.79 0.72 – 0.83 0.72 – 0.86 0.90-1.02 LDL-C, per 32.5 mg/dl Non-HDL-C, per 42mg/dl Apo B, per 29mg/dl HDL-C, per 14.7 mg/dl Apo A-I, per 29mg/dl TG, per 60% change Adjusted for confounding factors and lipid markers The Emerging Risk factors Collaboration JAMA 2009;302;1993-2000
Recommendations for lipid analyses astreatment target in the prevention of CVD
- - - CO2 CO2 CO2 STATINS VARY IN CHEMICAL STRUCTURES HO CO2Na HO CO2Na OH OH O HO O O F O O N O HO Simvastatin Fluvastatin Pravastatin HO HO - - HO OH OH OH F F F N Ca2+ Ca2+ Ca2+ O N N HN N N O2 Cyclopropyl Group 2 2 2 Pitavastatin Atorvastatin Rosuvastatin • Ose L Clin Lipidol 2010;5(3):309–323.
ACS Pravastatin L-CAD PACT Simvastatin A to Z Atorvastatin MIRACL PROVE IT-TIMI 22 Primary Prev Pravastatin WOSCOPS PROSPER Simvastatin HPS Atorvastatin ASCOT CARDS Rosuvastatin JUPITER Lovastatin TEXCAPS/AFCAPS The Evidence for Clinical Benefit of Statin Therapy for the prevention of CAD Secondary Prev Pravastatin • CARE • LIPID • PROSPER Simvastatin • 4S • HPS • SEARCH Atorvastatin • AVERT • TNT • IDEAL
Cholesterol Trialist CollaborationMeta-Analysis of Dyslipidemia Trials 50% 40% 30% 20% 10% 0% -10% Major Vascular Events Proportional reduction in event rate (SE) 0.5 1.0 1.5 2.0 Reduction in LDL cholesterol (mmol/L) CTT Collaborators. Lancet. 2005; 366:1267-78
CTT Collaboration Effects on Major Coronary Events per mmol/L LDL Cholesterol Reduction Subdivided by Baseline Lipid Values Heterogeneity/trend p-value Events (%) RR & CI Groups (mmol/L) Treatment Control (Treatment : Control) Total cholesterol: ≤5.2 748 (6·9) 940 (8·6) p = 0·7 5.2-6.5 1678 (7·0) 2246 (9·4) >6.5 896 (8·8) 1220 (12·1) LDL cholesterol: ≤3.5 1130 (6·8) 1443 (8·7) 3.5-4.5 1374 (7·3) 1814 (9·6) p = 0·5 >4.5 801 (9·3) 1120 (12·9) HDL cholesterol: ≤0.9 1167 (9·3) 1538 (12·1) p = 0·8 0.9-1.1 939 (7·4) 1270 (10·2) >1.1 1207 (6·2) 1595 (8·1) Triglycerides: ≤1.4 1162 (7·3) 1521 (9·6) 1.4-2.0 937 (7·1) 1304 (9·8) p = 0·6 >2.0 1217 (7·9) 1564 (10·2) 0·77 (0·74 – 0·80) Overall 3337 (7·4) 4420 (9·8) p < 0·00001 • 23% risk reduction per 39 mg/dl lowering of LDL-C - irrespective of • base line lipid levels • Starting statin therpay early in patients proves beneficial 0·5 1·0 1·5 Treatment Control better better CTT Collaborators. Lancet. 2005; 366:1267-78
No threshold of baseline LDL-C for benefit from intensive statin therapy • Statin doses which reduce LDL-C by 50% offer further benefit compared to doses which offer 20-30% reduction CTT 2 – Lancet 2010
4 Statin Benefit Groups IA IA IB IA IIaB
4 Statin Benefit Groups (continued) IA IA *10-year ASCVD Risk Calculator online
2013 ACC/AHA Essentially recommend either high intensity or moderate intensity statin treatment. High intensity statin treatment reduces LDL-C by around 50% (Atorvastatin 40 or 80mg, Rosuvastatin 20/40 mg) Moderate intensity statin treatment reduces LDL-c by 30-50% (Atorvastatin 10mg, Simvastatin 20 or 40mg, Pravastatin 40mg, Fluvastatin 40mg bd, Rosuvastatin 5 and 10mg) Considered risk reduction with either high or moderate intensity statin regimes with estimates of adverse events ▪ new onset DM (0.1/100 patient years with moderate intensity and 0.3/100 patient years with high intensity) ▪ myopathy ▪ haemorrhagic stroke No evidence of statin benefit if NYHA Class II-IV heart failure, or if on haemodialysis.
2011 ESC/EAS Treatment Targets Primary target: on treatment LDL-c Very high risk LDL-c < 70 MG/dL and or 50% ↓ in LDL-c when target level cannot be reached (Class I, Level A) High risk LDL-c < 100 mg/dL should be considered (Class IIa, Level A) Moderate risk LDL-c < 130 mg/dL should be considered (Class IIa, Level C) Secondary targets: non-HDL-c Very high risk < 100 mg/dL High risk < 140 mg/dL Apo B-100 Very high risk < 80 mg/dL High risk < 100 mg/dL
RISK OF ANY MAJOR VASCULAR EVENT IN PRIMARY PREVENTION • In low risk individuals less than 1%/ yr, 39 mg/dl reduces risk by 39% • Identify risks and start early with statin therapy CTT Lancet 2012
Loss-of-Function PCSK9 Mutations in AA Are Associated with Low LDL-C and Low Prevalence of CHD Events No Nonsense Mutation (N = 3278) 50th Percentile 30 20 10 0 Mean 138 mg/dL 88% reduction in the risk of CHD events during 15-year follow-up 12 8 4 0 9.7% 0 50 100 150 200 250 300 Frequency (%) Coronary Heart Disease (%) PCSK9142x or PCSK9679X (N=85) 30 20 10 0 Mean 100 mg/dL (-28%) 1.2% No Yes 0 50 100 150 200 250 300 PCSK9142x or PCSK9679X Plasma LDL Cholesterol in Black Subjects (mg/dL) • Life long lower LDL-C levels gives greater benefits than lowering LDL-C later on. Adapted from Cohen JC. N Engl J Med 2006;354:1264-72 ARIC=Atherosclerosis Risk in the Community
Screen early, treat early, think about lifetime risk 54.5 % relative risk reduction per 1 mM/L (38.7mg/dl) LDL-C lowering 22 % relative risk reduction per 1 mM/L (38.7mg/dl) LDL-C lowering 30% Major vascular events 50% Proportional reduction in event rate (SE) 40% rs11591147 20% 30% rs4420638 Proportional Risk Reduction (SE) rs6511720 20% rs646776 rs599839 rs2228671 10% 10% rs12916 rs11206510 0% rs4299376 1.0 2.0 0.5 1.5 -10% Reduction in LDL cholesterol (mmol/L) 0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0 11.0 12.0 13.0 14.0 15.0 16.0 17.0 18.0 Lower LDL-C (mg/dl) Ference BA et al. J Am Coll Cardiol 2012;60:2631–2639; Baigent C et al. Lancet 2005;366:1267–1278
PROVE IT Safety Results: Side Effects Wiviott, et al. JACC. 2005
Safety Results: Additional Features KM Estimates Opthalmologic AE Suicide/Trauma P (trend) = 0.31 P (trend) = 0.27
Relative Risk of Onset of Cancer from the Cholesterol Treatment Trialists' (CTT) Meta-Analysis of Statin Trials, According to Year of Onset Peto R et al. N Engl J Med 2008;359:1357-1366
Statins increase risk of Dysglycaemia Sattar N, Preiss D Ray, KKet al. Lancet 2010; 375: 735-42
Atorvastatin 80mg vs. Simvastatin 80mg Preiss ....Ray. JAMA 2011;305:2556-64
Risk of T2DM with Atorvastatin is Strongly Correlated to the Presence of Risk Factors (TNT) Waters et al. J Am Coll Cardiol 2011;57:1535-1545.
Prognosis of Patients with New-Onset T2DM Waters DD et al. JACC. 2011;
Absolute risk of cardiovascular disease over 5 years in patients by systolic blood pressure at specified levels of other risk factors Incremental Risk Diabetic, Smoker, Male, 60 yrs, TC : 240 mg/dl and HDL: 40MG/DL 44% 33% Reference Non Diabetic, Non Smoker, female, 50 yrs, TC : 160MG/dl and HDL: 60MG/DL 24% 18% 12% 6% 3%
CEPHESUS • Half of patients achieved LDL-C goals (49.1%); the other half (50.9%) failed to reach their LDL-C goals with existing treatment.
CEPHESUS • Nearly half (44.1%) of patients sometimes forget to take their tablets. About half (52.2%) of them forgot to take their tablets once every two weeks or more often. • About half (54%) of the patients thought missing a tablet once every two weeks or more often would not affect their cholesterol levels.
CEPHESUS • Physicians don’t like to switch treatment regimens; patients don’t like to be switched • 64.1% of patients still on same lipid-lowering drug since first prescribed.
Percentage reduction of LDL-C requested toachieve goals as a function of the starting value
Relationship between increase in HDL and atherosclerosis on IVUS Nicholls et al JAMA
Relationship Between Disease Burden and Cardiovascular Events Death, myocardial infarction and coronary revascularization Nicholls J Amer Coll Cardiol 2010
Summary • ESC guidelines identify 5 groups for CVD, DM, FH, high global risk • LDL-C targets depend on hisk with lower targets for those at highest risk • Statins are safe and currently the most effective treatments and pitavastatin has an excellent profile on LDL-C and HDL-C • Statins as a class seam to raise blood glucose in some but the benefits outweigh the risks. Pitavastatin may be the most glucose “gentle” in that regard