Download

1 / 28
380 likes | 602 Views
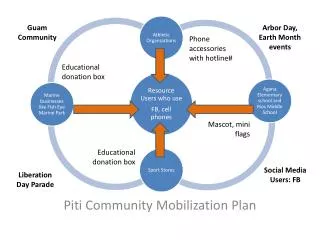
Community Mobilization. Seven Strategies to Affect Community Change. Provide information Seminars/workshops 2. Enhance skills As above 3. Provide support Enable attendance 4. Enhance access/reduce barriers May be reversed

E N D
Seven Strategies to Affect Community Change Provide information Seminars/workshops 2. Enhance skills As above 3. Provide support Enable attendance 4. Enhance access/reduce barriers May be reversed Change consequences Reward positive and punish negative behaviors 6. Change physical design Parks, lighting etc. 7. Modify and change policies Laws and policies U. of Kansas Work Group
Emerging Drug Items Identified in U.S. NFLIS Tox Labs: 2010 – 1/2 2012 (1/2 2012 incomplete) 7 SOURCE: U.S. DEA, Office of Diversion Control, NFLIS data, 2012.
Synthetic Drugs Will Turn You into a Zombie? TRAINER’S NAME TRAINING DATE TRAINING LOCATION
Synthetic Cannabinoids: The Major Compounds b) Cyclohexylphenoles a) Naphthoylindoles CP-47,497-C8 JWH-073 JWH-018 JWH-200 JWH-398 JWH-015 JWH-081 JWH-210 JWH-122 JWH-007 JWH-019 JWH-020 AM-2201 AM-1220 JWH-387 5-Fluoropentyl-JWH-122 JWH-412 10 SOURCE: Agudelo et al. (2012). Effects of Synthetic Cannabinoids on the Blood Brain Barrier, Presented at 74th Annual CPDD.
Synthetic Cathinones:“Bath Salts” • Could be MDPV, 4-MMC, mephedrone, or methylone • Sold on-line with little info on ingredients, dosage, etc. • Advertised as legal highs, legal meth, cocaine, or ecstasy • Taken orally or by inhaling • Serious side effects include tachycardia, hypertension, confusion or psychosis, nausea, convulsions • Labeled “not for human consumption” to get around laws prohibiting sales or possession 11 SOURCE: Wood & Dargan. (2012). Therapeutic Drug Monitoring, 34, 363-367.
Designer Drugs Bath salts The number of calls to poison centers concerning "bath salts" rose from 304 in 2010 to 6,138 in 2011, according to the American Association of Poison Control Centers. More than 1,000 calls had been made in 2012 by June. [8] Synthetic Marijuana In addition to K2 and Spice, other street names include Black Mamba (Turnera diffusa), Bombay Blue, Fake Weed, Genie, and Zohai.[9] According to Partnership at Drugfree.org, other names also include Bliss, Blaze, JWH -018, -073, -250, Yucatan Fire, Skunk and Moon Rocks.[13]
What isDXM? Dextromethorphanis a psychoactive drug found in common over the counter cough medicines. 13 SOURCE: NIDA. (2001). NIDA Research Report Series: Hallucinogens and Dissociative Drugs.
The Risk-Benefit Framework:Judge the Treatment, not the Patient INAPPROPRIATE • Is the patient good or bad? • Does the patient deserve pain meds? • Should this patient be punished or rewarded? • Should I trust him/her? APPROPRIATE Do the benefits of this treatment outweigh the untoward effects and risks in this patient or to society?
What Is the Addiction Risk? Published rates of abuse and/or addiction in chronic pain populations are 3-19%1 Suggests that known risk factors for abuse or addiction in the general population would be good predictors for problematic prescription opioid use Past cocaine use, history of alcohol or cannabis use2 Lifetime history of substance use disorder3 Family history of substance abuse, a history of legal problems and drug and alcohol abuse4 Heavy tobacco use5 History of severe depression or anxiety5 1 Fishbain et al. Clin J Pain, 1992; 2 Ives et al. BMC Health Services Research, 2006; 3 Reid et al. JGIM, 2002; 4 Michna el al. JPSM, 2004; 5Akbik H., et al. JPSM, 2006.
When Are Opioids Indicated? Pain is moderate to severe Pain has significant impact on function Pain has significant impact on quality of life Non-opioid pharmacotherapy has been tried and failed Patient agreeable to close monitoring of opioid use (e.g., pill counts, urine screens)
Opioid Efficacy in Chronic Pain Pain relief modest Some statistically significant, others trend toward benefit One meta-analysis decrease of 14 points on 100 point scale Limited or no functional improvement Most literature surveys & uncontrolled case series Randomized clinical trials (RCTs) are short duration < 4 months with small sample sizes < 300 pts Mostly pharmaceutical-company sponsored Balantyne JC, Mao, J. N Engl J Med, 2003.Martell et al. Ann Intern Med, 2007; Eisenberg et al. JAMA, 2005.
Opioid Dependence vs. Chronic Pain Managed with Opioids? The diagnosis of Opioid Dependence requires 3 or more criteria occurring over 12 months Tolerance – YES Withdrawal/physical dependence – YES Taken in larger amounts or over longer periods – MAYBE Unsuccessful efforts to cut down or control – MAYBE Great deal of time spent to obtain substance – MAYBE Important activities given up or reduced – MAYBE Continued use despite harm – MAYBE American Psychiatric Association. DSM IV-TR, 2000.
FAX CESAR November 19, 2012 Vol. 21, Issue 46 A Weekly FAX from the Center for Substance Abuse Research U n i v e r s i t y o f M a r y l a n d , C o l l e g e P a r k Alcohol Reported as Primary Substance of Abuse in 62% of Veterans’ Treatment Admissions There were nearly 58,000 admissions of veterans to substance abuse treatment facilities in 2010, according to the most recent data from the Treatment Episode Data Set (TEDS). TEDS, a database of treatment admissions to primarily publicly-funded substance abuse treatment facilities, excludes admissions to Veterans Affairs (VA) facilities. Therefore, the veteran admissions in TEDS represent veterans who chose to seek substance abuse treatment in a non-VA facility.* While alcohol was most likely to be reported as the primary substance of abuse among veterans and nonveterans alike, veterans were much more likely than nonveterans to report alcohol as their primary substance of abuse (62% vs. 42%). Veterans were less likely than nonveterans to report marijuana (7% vs. 15%) or heroin (8% vs. 16%) as their primary substance of abuse. No other substance besides alcohol was reported by more than 10% of veterans as a primary substance of abuse, suggesting that use prevention, intervention, and treatment programs for military personnel and veterans should focus their resources on alcohol. Primary Substance of Abuse in Treatment Admissions Ages 18 and Older, by Veteran Status, 2010 (N=57,934) *It is possible that veterans receiving treatment from VA treatment facilities may have a different pattern of primary substances of abuse than those found in TEDS. NOTES: A veteran is defined by TEDS as a person 16 years or over who has served (even for a short time), but is not now serving, on active duty in the US Army, Navy, Marine Corps, Coast Guard, or Commissioned Corps of the US Public Health Service or National Oceanic and Atmospheric Administration, or who served as a Merchant Marine seaman during World War II. Persons who served in the National Guard or Military Reserves are classified as veterans only if they were ever called or ordered to active duty, not counting the 4-6 months for initial training or yearly summer camps. SOURCES: Adapted by CESAR from Substance Abuse and Mental Health Data Archive (SAMHDA), online analysis of the concatenated1992-2010 Treatment Episode Data Set (TEDS), based on data received through 10/10/11, conducted 11/14/12 (available online at http://www.icpsr.umich.edu/icpsrweb/SAMHDA); andSubstance Abuse and Mental Health Services Administration (SAMHSA), Center for Behavioral Health Statistics and Quality, “Half of Substance Abuse Treatment Admissions among Veterans Aged 21 to 39 Involve Alcohol as the Primary Substance of Abuse,” Data Spotlight, November 8, 2012 (available online at www.samhsa.gov/data/2k12/TEDS2010N/TEDS2010NWeb.pdf). 301-405-9770 (voice) 301-403-8342 (fax) CESAR@umd.edu www.cesar.umd.edu CESAR FAX may be copied without permission. Please cite CESAR as the source.
Veterans, PTSD, and Substance Use Disorders • More than two of ten Veterans with PTSD also have SUD. • Almost one out of every three Veterans seeking treatment for SUD also has PTSD. • In the wars in Iraq and Afghanistan, about one in ten returning soldiers seen in VA have a problem with alcohol or other drugs. • New research from the University of Michigan suggests that veterans battling post-traumatic stress (PTSD) and substance abuse disorders face a greater risk of death.
Primary Substance of Abuse in Treatment Admissions Aged 21 to 39, by Veteran Status: 2010 Percent 40 20 60 50 30 10 0 50.7 34.4 Alcohol 9.0 Heroin Other Opiates 16.8 1 7.6 12.2 12.0 12.2 Marijuana Meth- amphetamine Crack 6.2 7.6 6.3 7.2 Veterans Nonveterans Cocaine/
Where to Go from Here http://www.healthquality.va.gov/Substance_Use_Disorder_SUD.asp The guideline describes the critical decision points in the Management of Substance Use Disorder and provides clear and comprehensive evidence based recommendations incorporating current information and practices for practitioners throughout the DoD and VA Health Care systems. The guideline is intended to improve patient outcomes and local management of patients with substance use disorder.
The guideline is formatted as five algorithms, with annotations: Algorithm A- Screening and Initial Assessment for Substance Use Disorder Algorithm B- Management of SUD in Specialty SUD Care Algorithm C- Management of SUD in (Primary) General Healthcare Algorithm P- Addiction-Focused Pharmacotherapy Algorithm S- Stabilization and Withdrawal Management