Download

1 / 23
230 likes | 348 Views
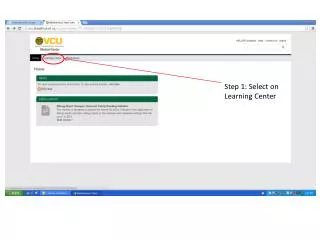
INFARTO MIOCARDICO RIDEFINITO Implicazioni epidemiologiche e socio-economiche Marcello Galvani Forlì. Learning Center ANMCO Firenze 1 ottobre 2001.

E N D
INFARTO MIOCARDICO RIDEFINITO Implicazioni epidemiologiche e socio-economiche Marcello Galvani Forlì Learning Center ANMCOFirenze 1 ottobre 2001
Report of the Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial InfarctionIII. DETECTION OF NECROSIS OF MYOCARDIAL CELLS • Infarcts are usually classified by size: • microscopic (focal necrosis), • small (<10% of the left ventricle), • medium (10% to 30% of the left ventricle), or • large (>30% of the left ventricle) Infarcts are classified temporally according to the pathologic appearance as follows: acute (6 h to 7 days); healing (7 to 28 days), healed (29 days or more).
50 20 10 5 2 1 Use of Cardiac Markers in ACS Early release myoglobin or CK-MB isoformsCardiac troponin after “classical” AMICK-MB after AMICardiac troponin after “microinfarction” Multiples of the AMI Cutoff Limit AMI decision limit Upper reference limit 0 1 2 3 4 5 6 7 8 Days After Onset of AMI From Wu AH et al. Clin Chem 1999;45:1104.
Report of the Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial InfarctionIII. BIOCHEMICAL DETECTION OF NECROSIS OF MYOCARDIAL CELLS • Specificità per la necrosi cellulare • Sensibilità di riconoscimento del danno miocardico • Specificità miocardica • Praticabilità della definizione biochimica
Myocardial Necrosis with negative Total CK,but with Positive Troponine T Bedside test . A, Transverse section of heart Anterior wall of left ventricle is at top and lateral wall is at right. Viable myocardium is magenta and necrotic myocardium is brown to gray. Hyaline white material is old scar. .B, Microscopic section from posterior left ventricular wallSmall arrows indicate area of coagulation necrosis consistent with microscopic infarct 12 to 36 hours old. C, Device for rapid bedside cTnT assay performed on whole blood from patient 16 hours after onset of chest pain and 12 hours before death.Dark line to left (c) is positive control, and fainterline to right (arrow) is positive patient result (when at least 0.2 ng/ml of cTnT is present). Antman EM, Am Heart J 1997
Intracellular Cardiac Marker Proteins and Their Compartmentation Cytosolic: GOT, LD (LD1,LD2), CK, CK-MB (Activity,“Mass” Concentration, Isoforms) Mgb, FABB, GP-BB Cytosolic + structural: cTnT 6% vs 94% cTnI 3% vs 97% Structural: Myosin LC Myosin HC Actin Free cTnT cTnT-I-C complex cTnT (g/L) cTnT fragments Retention Time (min) cTnI-C complex Wu, Clin Chem 1998;44:1198 cTnT-I-C complex cTnI (g/L) Retention Time (min) = “New” Markers cTnT-I-C complex 77kDa free cTnT 33kDa free cTnI 27kDa =“Early” Markers =“Conventional” Markers
SENSIBILITA’ DEI MARCATORI DI DANNO MIOCARDICO 108 pazienti con S.C.A. senza I.M.A. classico Anno di comparsa del test 1991 +32% 1979 +5% 1985 +12% 1970 % Pazienti
Specificità della Troponina per la Necrosi Miocardica: Elevazioni in Assenza di IMA Definito Secondo i Criteri WHO • Angina Instabile • Miocardite e Pericardite • Scompenso Cardiaco • Cuore Polmonare Acuto • Contusione Miocardica • Tossicità Miocardica da Chemioterapici • Rigetto nel Trapianto Cardiaco • Insufficienza Renale (?)
Interferenze Analitiche con il Dosaggio della Troponina I • Falsi positivi: • Fibrina • Fattore reumatoide • Anticorpi eterofili • Falsi negativi: • Bilirubina elevata • Anticorpi circolanti anti-troponina I
Praticabilità della definizione biochimica di IMA(consigli per il cardiologo) • Collaborare con il Laboratorista al fine di: 1) analizzare le caratteristiche del metodo scelto per la misurazione della Tn (TnT vs. TnI, etc.); 2) arrivare a definire il 990 percentile della popolazione di controllo (se non già definito nel foglietto illustrativo); 3) definire il livello al quale il metodo assicura un CV 10%; 4) utilizzare questo livello come diagnostico di IMA se significativamente più elevato del precedente.
Implications of different definitions of MIReport of the Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction • Epidemiologia • Trial Clinici • Singolo paziente • Gestione della salute pubblica EHJ/JACC September 2000
Epidemiologia Epidemiological classification of acute myocardial infarction: time for a change?P. Porela, H. Helenius, K. Pulkki, L.-M. Voipio-PulkkiEur Heart 1999;20:1459-1464 Editorial It’s Time for a Change to a Troponin Standard Allan S. Jaffe, MD; Jan Ravkilde, MD, DMSc; Robert Roberts, MD; Ulf Naslund, MD, PhD; Fred S. Apple, PhD; Marcello Galvani, MD; Hugo Katus, MD, PhD Circulation. 2000;102:1216-1220
Definizione “epidemiologica” vs. “biochimica” di IMA Porela et al, Eur Heart J 1999;20:1459-1464
Trial Clinici • There have been different thresholds for identifying • an infarct in trials undertaken up to this time in the • U.S.: • . CK-MB x2 times the upper limit of normal (ULN) for spontaneous MI; • . CK-MB x3 times the ULN with coronary • artery interventions; • . CK-MB x5 to 10 times the ULN for bypass surgery. EHJ/JACC September 2000
PROGNOSI DELLE SINDROMI CORONARICHE ACUTE Unstable angina according to troponin results Death or MI (%) FRISC Study Death or MI (%) TRIM Study Death (%) TIMI IIIB Study
Relation Between cTnT and EF in AMI 40 35 30 25 20 Troponin T (g/L) 15 10 5 0 0 10 20 30 40 50 60 70 80 Ejection Fraction (%) Rao ACR et al, Heart 1998;80:223
MINISTERO DELLA SANITA’Tabella delle percentuali d’invalidità per le minorazioni e malattie invalidanti 26-2-1992 Supplemento ordinario alla GAZZETTA UFFICIALE Serie generale - 47
TARIFFE DELLE PRESTAZIONI DI ASSISTENZA OSPEDALIERA PER ACUTI EROGATE IN REGIME DI RICOVERO ORDINARIOACFA-DRG Versione 100Regione Emilia-Romagna anno 2000(Importi in migliaia di lire) RIMBORSO PESO 3.203 6.170 3.907 0.6219 1.2029 0.7587 140 M-Angina pectoris 124 M-Malattie cardiovasc. no IMA, con cateterismo card. e diag.CC 125 M-Malattie cardiovasc.eccetto IMA, con cateter.card.diag.no CC 121 M-Malattie cardiovascolari con IMA con compl.cardiovasc. vivi 10.023 7.983 7.916 1.6114 1.1532 1.4090 122 M-Malattie cardiovascolari con IMA no compl. cardiovasc. vivi 123 M-Malattie cardiovascolari con IMA, deceduti
AICare-2 Costi dell’aumento del numero di D.R.G. per IMA Ricoveri annuali per SCA in Emilia Romagna ~ 12.000 pazienti/anno ricoverati(80% in UTIC o Cardiologia) 5040 (42%)IMA-Q 3240 (27%)IMA-non Q 3720 (31%)AI - 1116 (30%)IMA AI + 9396 (78%)IMA 2604 (22%)AI *Differenza: L 3.500.000/ricovero *20% diagnosi complicate, 50% coronaro e 20% PCI nell’AI
Pazienti IMA non Q Costi complessivi (£. #.000.000) AICare-2
Pazienti con Angina instabile Costi complessivi (£. #.000.000) AICare-2