Download
1 / 68
680 likes | 981 Views
Infected Total Hip/Knee Arthroplasty. Kristi Wood April 5, 2012. Objectives. Overview of infections after THA/TKA Diagnosis Management. History. The modern era of arthroplasty is about 35 years old Initial series showed infection rates around 9%

E N D
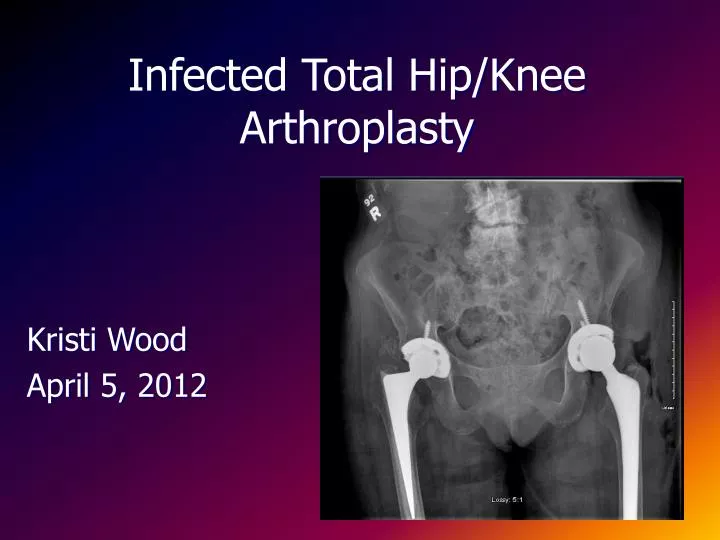
Infected Total Hip/Knee Arthroplasty Kristi Wood April 5, 2012
Objectives • Overview of infections after THA/TKA • Diagnosis • Management
History • The modern era of arthroplasty is about 35 years old • Initial series showed infection rates around 9% • Improvements in air quality in the OR, prophylactic antibiotics, and patient selection have greatly decreased those rates
Economics • US figures indicate that average cost of revision is $50 000 to $60 000 • 3500 – 4000 infected THA per year • Total cost $150 -$200 million per year
Incidence of Infection • Reports in the literature range from: • 0.3% (British Medical research council trial) • 2.2% (US Medicare data 1986-1989) • Some evidence that dedicated institutions with large numbers of THA yearly have lower infection rates ~ 1%
Incidence • Mayo Clinic data – 1969-1996
Incidence • Patient factors • OR environment • Surgical factors and technique • Perioperative care
Patient Factors • Rheumatoid arthritis – OR ~ 4 • Diabetes – OR ~ 2 • Sickle cell anemia – 23% • Psoriasis – superficial infection 9.1% deep infection 5.5% • Renal or liver transplantation – 19% • ESRD on dialysis – 13% • Poor nutrition has been implicated in delayed wound healing but has not been correlated with deep infection
Surgical Factors • Increased incidence after revision surgery • 3.2% vs 1.3% in Mayo clinic study for THA • Any previous surgery • 2.3% vs 0.9% for THA • 0.3 % vs 1.4% in pts with OA for TKA (Wilson et al) • Revision for aseptic loosening – 2.5% • Revision with previous infection – 4% • Revision with structural femoral allograft – 5% • Conversion of arthrodesis to THA – 10-13% • Large hinged TKA – 11-16%
Surgical Factors • Operative time • Avoid dead space and hematoma formation • Minimize tissue trauma • exposes collagen and basement membrane proteins to the bloodstream which enhances bacterial binding to fibronectin (esp S. aureus)
Perioperative Care • Systemic antibiotics • Hill et al – double blind RCT on 2137 THA showed reduction in infection from 3.3% (placebo) vs 0.9% (5 days cefazolin) • Nelson et al – demonstrated equal efficacy for 1 day vs 7 days of antibiotics in a randomized trial of 358 patients • Many other similar studies but power is an issue • Classen et al – large prospective trial showed lowest rate of wound infections with antibiotics given 2 hrs before incision vs just after incision or more than 2 hrs before incision • Recommendations • ancef 1 g iv 15-30 minutes preop followed by 2-3 postoperative doses • Further doses intraoperatively if blood loss >2L or >4hrs operative time • Vancomycin 1g iv for anaphylactic penicillin allergy only followed by one postoperative dose
Perioperative Care • Drains • Willett et al – prospective study of 120 THA • Drain removed at 24, 48 or 72 hours • 90.9% of total blood loss in first 24 hours • Seven positive deep wound cultures all in pts with drain removed at 48 or 72 hrs • All deep cultures had growth of identical organisms on pts skin • Beer et al – prospective study of bilateral THA (24) and TKA (76) • No difference in swelling or persistent wound drainage • Kim et al – prospective study of 96 bilateral THA • Significant increase in wound drainage and erythema in the undrained hips • No difference in infection rates or functional outcomes at 1 year • Recommendations • Remove drain at 24 hrs in most situations
Perioperative Care • Persistant wound drainage • No evidence to support use of prolonged antibiotics with persistant serous drainage • Permits overgrowth of antibiotic resistant organisms • Recommendations • Avoid prolonged postoperative Abx • Compressive bandages and minimize activity to allow wound to seal • If drainage persists >5-7 days wound debridement and tissue samples for culture allow for possible prosthesis retention if due to infection
Perioperative Care • Urinary Retention • Wroblewski et al reported 6.2% deep infection rate in 195 men with postoperative urinary retention vs overall rate of 0.5% • 59% of those who required catheterization received antibiotic coverage • Foley removed 24-48 hrs post op has been shown to decrease urinary retention while not increasing UTI • Recommendations • Pts with urologic symptoms should have them treated prior to THA • Antibiotic prophylaxis should be given for urinary tract manipulation in the postoperative period
Routes of Infection • Direct contamination during OR • Direct or contiguous spread • Hematogenous spread • Reactivation of previous infection
Routes of Infection • Operating Room Environment • Each person in the OR will shed 1000 - 10 000 bacteria/min • Average OR has 300-400 colony forming units (cfus) per sq ft/hr • Attempts to decrease cfus: • Horizontal laminar air flow – 93% reduction in airborne bacteria • decreased infection rates from 1.4% to 0.9% in THA • increased infection rates from 1.4% to 3.9% in TKA. • Body exhaust suits • no difference in bacterial counts when used with laminar air flow • 80% reduction vs regular scrubs • HOWEVER: Retrospective review - The rate of revision for early deep infection NOT reduced by using laminar flow or space suits. • Hooper et al. JBJS Br 2011Ten year results of New Zealand Joint Registry)
Routes of Infection • Operating Room Environment • Face masks – wearing a surgical face mask in the sterile core and/or the OR had no effect on the bacterial counts in either the core or the OR • Head cover – no statistically significant difference between no head cover, caps or hoods • Contaminated gloves (29%), suction tips (33%), skin blades(9%), needles(10%), surgical gowns(17%), light handles(14%) • UV light – infection rate of 0.5% for 2389 hips but all OR personnel must be protected from burns
Routes of Infection • Direct Spread • Organisms migrate to the hip joint from a more superficial infection • Schmalzried et al – series of 3051 hips with 47 deep infections – 2/47 by direct spread from superficial infection • Surin et al – series of 803 hips with 34 deep infections – increased risk (3.2X) if there was increased postoperative wound drainage • Gaine et al – series of 301 hips had no deep infections despite 56 superficial infections
Routes of Infection • Direct Spread • Skin necrosis is an issue for TKA • Previous incisions should be used if possible or a minimum 7 mm skin bridge • 25% of TKA may have prolonged wound drainage • In pts with tense knee effusion, persistent significant pain – I&D early
Routes of Infection • Hematogenous spread • Skin infections – remote from incision • Dental infections • Dental manipulation • Urinary tract infections • Reactivation • Reactivation of infection in a previously infected hip or knee
Antibiotic prophylaxis for bacteremia • Case reports of hematogenous seeding of THA following dental procedures • Current recommendations of the AAOS • Prophylactic Abx recommended 1 hour prior to dental procedures • Especially for Immunocompromised pts, RA, SLE, diabetes, hx of infected THA, malnourishment, hemophilia, medical comorbidities (HIV, obesity, diabetes, smoking), malignancy • Amoxicillin, cephradine or cephalexin 2 g PO or ancef 1 g iv (or clindamycin 600mg po/iv if penicillin allergic) 1 hour prior to dental procedure
American Dental Association opinion … 1997 through 2006 from the Medicare Current Beneficiary Survey (MCBS)…. explored associations between dental infections and subsequent PJI. Dental procedures were not associated significantly with subsequent risk for PJIs … power was somewhat low. CONCLUSION Antibiotic prophylaxis … should be reconsidered for patients in that population who are receiving oral health care
Classification of Periprosthetic Hip or Knee Infections - Fitzgerald • Fitzgerald et al • Stage I – acute fulminant infection • Within 3 months of surgery • Present with systemic symptoms – fever, chills, sepsis and unremitting pain even at rest • Wound drainage, erythema, swelling or abscess • Stage II – delayed sepsis • Indolent infection within 2 years of surgery • May originate at time of OR but presentation delayed due to small inoculum or low virulence of infecting organism • Most common and most difficult to treat • Stage III – late hematogenous • Metastatic infections caused by hematogenous spread • Symptoms of acute infection similar to stage I in a previously asymptomatic THA • Seeding can occur regardless of status of fixation of the components
Classification of Periprosthetic Hip or Knee Infections - Tsukayama • Early postop - onset within first month after surgery • Late chronic infection - onset more than 1 month after surgery, insidious onset of symptoms • Acute hematogenous infection - onset > 1 month after surgery, acute onset of symptoms in previously well-functioning prosthesis, distant source of infection • Positive intraoperative cultures - positive cultures obtained at the time of revision for supposedly aseptic conditions
Bacteria • Infecting organisms can be divided into • Planktonic – individual free floating cells • Usually early after inoculation • Easier to eradicate • Sessile – biofilm of glycocalyx • Can adhere to and survive on synthetic surfaces and are protected from antibiotics, complement activation and ingestion by neutrophils • Most bacteria in the correct environment can form a biofilm • Requires time to form after inoculation • Stable prostheses covered with living tissue are less vulnerable to adherence and biofilm formation
Bacteria • Biofilm producers • S. aureus • S. epidermidis • pseudomonas • Poor Biofilm producers • Gram negatives (except pseudomonas)
Bacteria • CONS and S. aureus are most common • then • Strep (not A or D), • Anaerobic strep+microaerophilic • Pseudomonas • E coli • Enterococcus • S. aureus predominant in early infections • Gram –ve: usually hematogenous, esp UTI • Mixed infections - when draining sinus Salvati EA, Della Valle AG, Masri BA, et al: The infected total hip arthroplasty, Instr Course Lect 52:223, 2003
Virulence and Resistance • Gram negative bacilli and Group D strep (enterococci) are considered more virulent organisms • S. epi is generally considered low virulence but may be difficult to eradicate due to glycocalyx - also this species is demonstrating increased antibiotic resistance • MRSA , VRE, methicillin resistant S. epi infections are becoming increasingly common
Susceptibility to Infection • Foreign bodies produce an inflammatory and necrotic tissue response • Response is greater with articulated implants and increases with high levels of wear debris • Polymethylmethacrylate has been shown to reduce chemotaxis, phagocytosis and killing ability of PMNs
Diagnosis of Infection • History • Risk factors • Persistent drainage or delayed wound healing • Constant pain • Early or late acute infections: • pain, fever, wound drainage, or erythema • Chronic infection: • Pain unrelieved by a seemingly well-functioning arthroplasty • Also worrisome: excessive wound drainage after initial arthroplasty, multiple episodes of wound erythema, and prolonged antibiotic treatment by the operating surgeon
Physical exam • Presence or absence of: • Painful hip range of motion • Swelling • Erythema • Sinus formation • Fluctuance
Laboratory Investigations • ESR • Measurement of red blood cells that have been caused to agglutinate by acute phase proteins • ESR>30mm/h - sensitivity 82%, specificity 85% (PPV – 58%, NPV 95%) for the diagnosis of infection • Elevated by other factors including concomitant infection, inflammatory arthritis, collagen vascular disease, recent surgical intervention (up to 12 months), malignancy • ESR>30mm/h 6 months after a two stage revision has a 62% chance of indicating persistent infection • May be useful as a monitoring tool
Laboratory Investigations • CRP • Acute phase protein which contributes to an elevated ESR • Returns to normal within 3 weeks of surgery with peak levels 2-3 days post op • CRP>10mg/L sensitivity 96% specificity 92% (PPV – 74% and NPV – 99%) • Normal ESR and CRP can reliably rule out infection • Abnormal ESR and CRP indicate 83% probability of infection
Laboratory Investigations • WBC • Rarely elevated in chronic infection • WBC > 11 • Sensitivity 20% • Specificity 96% • PPV 50% • NPV 85%
Radiographic Investigations • Plain xrays • Often normal in the early stages of infection • Subtle findings may be present • Periosteitis • Localized osteopenia • Endosteal scalloping • Ring osteolysis around wires and cables • Loosening may or may not be associated with infection
Periosteal new bone formation • Focal osteolysis at tip • Faint periosteal elevation
Radiographic Investigations • MRI • Presence of signal loss adjacent to the metal components • Titanium less ferromagnetic than Co-Chromium • Can show periprosthetic abscesses or intrapelvic extension • US • Can also be used to detect abscesses and for US guided aspiration of hip/abscess for diagnosis • Thickened capsule may indicate infection
Radiographic Investigations • Radionuclide Scans • bone scan is sensitive but not specific • Normal scan should rule out infection or loosening • Abnormal in both infection, loosening, for up to 1 year post operatively, heterotopic ossification, inflammatory conditions, fractures and tumours • WBC scans are sensitive at diagnosing conditions with increased vascularity and WBC uptake but can be negative in chronic infection due to poor uptake • PPV – 54-63%, NPV – 95% • Better accuracy with combination WBC/bone scan
Invasive Diagnostic Tests • Aspiration • Can confirm the presence of infection and identify the organism(s) involved and antibiotic sensitivities • Should be done prior to administration of antibiotics or two weeks since last dose • Sensitivity 92%, specificity 97%, accuracy 96% • Gram stain, cell count, glucose, protein, lactic acid? • If cell count >25 000 leukocytes/ml and >25 % PMNS infection suspected • Allows arthrogram at the same time
Hip Arthrogram • Deep delayed infection in 84 yo man • Acetabular migration • Long sinus tract extending posterior to femoral shaft
Emerging Molecular Biological Techniques • A single-center study • serum IL-6 level is very sensitive and specific for periprosthetic infection • But further studies required • Serologic markers for specific infections
Intraoperative Tests • Grossly abnormal tissues at time of revision surgery despite a negative workup - sensitivity 70% and specificity 87% • Send immediate gram stain • Sensitivity 19%, specificity 98%, PPV 63%, NPV 89% • Culture of synovial fluid • Frozen section of inflamed tissue >5 PMNs per hpf • Sensitivity 80-100% specificity 94-96% • Intraoperative Cultures • Gold standard - sensitivity 94%, specificity 97%, PPV 77%, NPV 99% • At least 3 tissue samples • Swab cultures from the removed implant are less sensitive
Algorithm for Infection • High index of suspicion • History and physical and xrays • ESR and CRP • If normal – no further tests (unless high index of suspicion) • If abnormal – aspiration • Aspirate • If normal but high index of suspicion • Repeat aspirate with arthrogram (hip) or US or biopsy • If all tests normal but high index • May resort to intraoperative methods • If frozen section negative – may proceed with revision
Treatment • Consists of one or more of the following • Antibiotic therapy • I+D with component retention • I+D with component removal • One-stage or two-stage reimplantation • Arthrodesis • Amputation
Treatment • Antibiotic suppression • Small series involving patients who were deemed to be unsuitable for reconstruction or who had refused reconstruction – 37% revision rate • May be an option for pts who refuse OR or are medically unsuitable • Infection should not produce systemic symptoms, prosthetic components should be well fixed, organism should be sensitive to po Abx
Treatment • Incision and drainage • Often used as initial treatment in acute early or late acute hematogenous infections • Retention rates in early acute infection – 26-71% • Retention rates in late acute hematogenous infection – 26-50% • Duration of symptoms correlates with success rates • Brandt et al – 56% retention if treated within 2 days • 13% retention if treated after 2 days of symptoms • All components must be well fixed, any loose components must be removed • Poly exchange • In chronic periprosthetic infection failure rate is 95-100%
Treatment • Excision Arthroplasty • Most predictable procedure to eradicate infection • consists of removal of the infected prosthesis and cement and débridement of the synovium • The bone ends can be temporarily apposed with heavy sutures or pins. • Bourne et al – 1/33 reinfection rate
Treatment • Excision Arthroplasty • Functional outcome is very poor including decreased active ROM and strength • O2 consumption higher than an AKA for THA • May allow for some ROM at knee but severely limits walking ability • Salvage procedure to provide some pain relief in patients not suitable for reconstruction
Reimplantation • Two Stage Exchange Arthroplasty • Provides a better environment for eradication of infection • Organisms may be cultured from tissue samples which allows for further microbiological assessment and adjustment of antibiotics • Goal is to prevent a complex reconstruction in the presence of unresolved sepsis