Download
1 / 16
280 likes | 1.65k Views
NUR 111: Skill 5-3: assessing apical pulse. The apical pulse is the most reliable non-invasive way to assess cardiac function. WHAT ELSE IS INCLUDED IN THIS POWER POINT PRESENTATION?. Brief description of procedural guideline 5-1: assessing apical-radial pulse

E N D
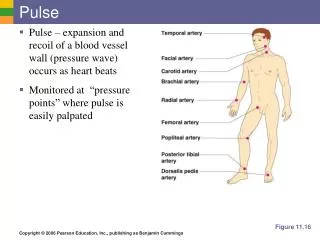
NUR 111: Skill 5-3: assessing apical pulse The apical pulse is the most reliable non-invasive way to assess cardiac function.
WHAT ELSE IS INCLUDED IN THIS POWER POINT PRESENTATION? • Brief description of procedural guideline 5-1:assessing apical-radial pulse • Skill 5-4: assessing respirations
ASSESSING APICAL PULSE • As with assessing the radial pulse, you will perform an ASSESSMENT: • Assess for any risk factors for apical pulse alteration: • Heart Disease • Cardiac Dysrhythmia • Onset of sudden chest pain or acute pain from any site • Invasive cardiovascular diagnostic tests • Surgery • Internal or external hemorrhage • Administration of medications that alter heart function
Assessment of apical pulse – cont’d • ASSESSMENT: CONT’D: • Assess for signs & symptoms of altered cardiac function, such as dyspnea, fatigue, chest pain, orthopnea, syncope, palpitations, edema or dependent body parts, cyanosis or pallor of skin. • Assess for factors that normally influence apical pulse rate, such as: Age; Exercise, Position Changes, Medications; Temperature; Sympathetic stimulation. • Determine previous baseline apical rate (if available) from patient’s record. • Determine any report of latex allergy; If patient has latex allergy ensure that stethoscope is latex free. • PLANNING: • Expected outcomes following completion of procedure: • Apical Heart Rate is within acceptable range. • Rhythm is regular • Explain to patient that you will assess apical pulse rate. Encourage patient to relax & ask them not to speak. If patient has been active, wait 5 to 10 minutes before assessing pulse. If they have been smoking or ingesting caffeine, wait 15 minutes before assessing their pulse.
IMPLEMENTATION • 1. Perform Hand Hygiene • 2. If necessary, draw curtain around bed and / or close door – provide privacy for the patient. • 3. Assist patient to supine or sitting position. Move aside bed linen and gown to expose sternum & left side of chest. • 4. Locate anatomic landmarks to identify point of maximal impulse (PMI), also called apical impulse. The heart is located behind & to the left of the sternum with base at top and apex at the bottom. • Find angle of Louis just below suprasternal notch between sternal body & manubrium: it feels like a bony prominence (CONT’D ON NEXT PAGE)
Implementation – cont’d • . Slip fingers down each side of angle to find second intercostal space (ICS). Carefully move fingers down left side of sternum to fifth ICS & laterally to left mid-clavicular line (MLC). A light tap felt within area 1 to 2.5 cm (1/2 to 1 inch) to PMI is reflected from apex of heart. • Use of anatomic landmarks allows correct placement of stethoscope over apex of heart. This position enhances ability to hear heart sounds clearly. If unable to palpate PMI, (Point of Maximal Impulse) reposition patient on left side.
Locate the point of maximal impulse at fifth intercostal space • Nurse locates sternal notch • Nurse locates second intercostal space • Nurse locates fifth intercostal space • Nurse locates point of maximal impulse at fifth intercostal space • Place diaphragm of stethoscope in palm of hand for 5 to 10 seconds. • Warming of metal or plastic diaphragm prevents patient from being startled and promotes comfort
Assessing apical pulse – cont’d • Place diaphragm of stethoscope over PMI at FIFTH ICS, at left MCL, and auscultate for normal S1 & S2 heart sounds (heard as “lub-dub”) • When you hear S1 & S2 with regularity, use second hand of watch and begin to count rate: when sweep hand hits number on dial; start counting with zero, then one, two & so on. • If apical rate is regular, count for 30 seconds & multiply by 2. • If HR (Heart Rate) is irregular or patient is receiving cardiovascular medication, count for a full 1 minute (60 seconds). • Note regularity of any dysrhythmia (S1 & S2 occurring early or late after previous sequence of sounds ) (e.g., every third or every fourth beat is skipped). • Replace patient’s gown & bed linen; help them return to comfortable position. • Clinical Decision Point: If apical rate is abnormal or irregular, repeat measurement or have another nurse conduct measurement. Original measurement may be incorrect. Second measurement confirms initial findings of abnormal heart rate.
END OF SKILL • This is the end of the skill! • While this power point presentation may be helpful, practice in the skills lab is priceless! • Here is the video link for this skill: • http://booksite.Elsevier.com/Perry-Potter/ClinicalSkills/video03.php • Elsevier:Perry-Potter: Clinical Nursing Skills and Techniques, 8e-5.3 Assessing Apical Pulse • Please watch this video & Practice the Skill in the Nursing Lab! • Find all of the points, i.e.; PMI, 5th intercostal space, Angle of Louis (just below suprasternal notch between sternal body & manubrium; Remember; it feels like a bony prominence • Slip fingers down each side of angle to find 2nd intercostal space • Carefully move fingers down left side of sternum to 5th ICS & laterally to left midclavicular line (MCL) • A light tap felt within area 1 to 2.5 cm (1/2 to 1 inch) of PMI is reflected from apex of heart
While this is the end of the skill, you will need to look over the unexpected outcomes • Unexpected Outcomes: • An adult patient’s apical pulse is greater than 100 beats per minute: (Tachycardia) • Patient’s apical pulse is less than 60 beats per minute: (Bradycardia) • Patient’s apical rhythm is irregular • Don’t forget to record & report the patient’s pulse
Brief description of procedural guideline 5-1:assessing apical-radial pulse • I will be giving a brief description of Performance Checklist Procedural Guideline: 5-1: Assessing Apical-Radial Pulse Page 85 in the 8th Edition of Clinical Nursing Skills & Techniques, Perry, Potter & Ostendorf • The difference between pulses assessed from two different sites, or a pulse deficit, provides information about heart and blood vessel function. • When a pulse deficit is assessed between the apical and radial pulses, the volume of blood ejected from the heart may be inadequate to meet the circulatory needs of the tissues, and intervention may be required. • To assess for a pulse deficit, the nurse & a second health care provider assess a peripheral pulse rate & the apical pulse rate simultaneously & compare the measurements. • NOTE THE TWO NURSES ABOVE!
ASSESSING APICAL-RADIAL PULSE: PROCEDURAL GUIDELINE 5-1 • I’m only going to go over this briefly, if you would like detailed information on this, please go to your book! • For the procedural steps: • Determine need to assess for pulse deficit. Irregular heart rate & signs & symptoms such as dyspnea, fatigue, chest pain & palpitations may indicate abnormal cardiac function. • Assist patient to supine or sitting position. • Locate apical & radial pulse sites. Nurse auscultates apical pulse, while 2nd provider palpates radial pulse • Nurse begins pulse count by calling out loud when to begin counting pulse. • Each nurse completes a 60 second pulse count simultaneously. The count ends when the nurse states “stop.” Sixty seconds is required when a discrepancy between pulse sites is expected or when the rhythm is irregular.
Skill 5-4: assessing respirations • What is RESPIRATION? • Respiration is the exchange of oxygen & carbon dioxide between cells of the body & the atmosphere. • During quiet breathing, the chest wall gently rises & falls. • I could type a hundred page paper about how to measure a patient’s respiration, but the only way to conquer this skill is PRACTICE! • To view this skill by video: here is the link: • http://booksite.Elsevier.com/Perry-Potter/ClinicalSkills/video04.php • Elsevier:Perry-Potter: Clinical Nursing Skills and Techniques, 8e-5.4 Assessing Respirations
Skill 5-4: assessing respirations cont’d • Again, I’m not going to go over this skill, in detail, as you need to watch the video & practice in the nursing skills lab in order to pass this skill. I will, however, discuss alterations in Breathing Pattern. This is Box 5-5 in your book. • ALTERATIONS IN BREATHING PATTERNS: • Apnea: Respirations cease for several seconds. Persistent cessations results in respiratory arrest. • Biot’s respiration: Irregular respirations vary in depth and are interrupted by periods of apnea. • Bradypnea: Rate of breathing is regular but abnormally slow (fewer than 12 breaths/min). • Cheyne-Stokes Respiration: Respiratory rate & depth are irregular, characterized by alternating periods of apnea & hyperventilation. Respiratory cycle begins with slow, shallow breaths that gradually increase to abnormal rate & depth. The pattern reverses; breathing slows & becomes shallow, climaxing in apnea before respiration resumes.
SKILL 5-4: ALTERATIONS IN BREATHING PATTERN – CONT’D • Hyperpnea: Respirations are increased in depth: occurs normally during exercise. • Hyperventilation: Rate & depth of respirations increase. Hypocarbia, an abnormally low level of carbon dioxide in the blood, may occur. • Hypoventilation: Respiratory rate is abnormally low; depth of ventilation may be depressed. Hypercarbia, an abnormally elevated level of carbon dioxide in the blood, may occur. • Kussmaul’s respiration: respirations are abnormally rapid and deep but regular; common id diabetic ketoacidosis. • Tachypnea: Rate of breathing is regular but abnormally rapid (more than 20 breaths/min).
Assessing arterial blood pressure: skill 5-5: will be on new power point presentation • For this skill, Please see a new power-point presentation. • Before you go: Please remember the following: • Remember, Blood pressure (BP) is the force exerted by blood against the vessel walls. • The peak pressure occurs when the ventricular contraction of the heart, or systole, forces blood under high pressure into the aorta. • Learning how to take a patient’s Blood Pressure is Vital, especially since Hypertension is known as the “SILENT KILLER!” • According to MedicineNet.com: Untreated hypertension increases the risk of heart disease & stroke. These are the first & third commonest causes of death in the USA. Hypertension can also damage the kidneys & increase the risk of blindness & dementia. This is why hypertension is referred to as a “Silent Killer.”