Download
1 / 36
360 likes | 512 Views
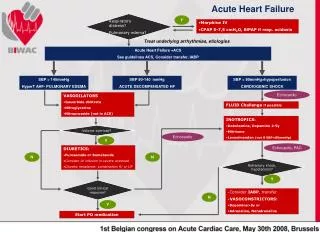
Managing Acute Heart Failure in the Emergency Department. Patient Case S tudy. Click on the icons for more information. Revised Diagnosis and Care Plan. Initial Diagnosis and Care Plan. Teaching Points Discussion and Conclusions. Case Introduction. 5. 1. 3. 7. Glossary. 6. 2. 4.

E N D
Managing Acute Heart Failure in the Emergency Department Patient Case Study Click on the icons for more information Revised Diagnosisand Care Plan Initial Diagnosis and Care Plan Teaching PointsDiscussion and Conclusions Case Introduction 5 1 3 7 Glossary 6 2 4 DispositionDecision ? Questions Case Details and Initial Triage DiagnosticResults Author: Peter S. Pang,MD, MS, FACEP, FAAEM FAHA, FACC
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Peter S. Pang, MD, MSc, FACEP FAAEM, FAHA, FACC • Indiana University School of Medicine(Indianapolis, IN; USA) • Associate Professor, Emergency Medicine • Associate Director, Clinical Research CASE INTRODUCTION More
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Background • It is 2 am. You are the only physician immediately available for the entire hospital in this small, 50 bed hospital located approximately 300 km from the nearest tertiary referral medical center. You are board certified in emergency medicine • Although the hospital is small, you have a full complement of nurses and you are skilled in bedside ultrasound. This is the only hospital within a 150 km radius • There is no point of care (POC) testing • There is no formal echo available within 6 hours CASE INTRODUCTION echo=echocardiogram
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Click on the icons for more information Past History, Allergy History, Medications, and Social History History of Present Illness and Review of systems HPI Chief Complaint and Vital Signs Physical Examination CASE DETAILS AND INITIAL TRIAGE Author: Peter S. Pang,MD, MS, FACEP, FAAEM FAHA, FACC
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Chief Complaint • “I can’t breathe” (states the patient) • Mode of arrival: EMS • Paramedics report a 71 year old female who called 911 at 1.15 am c/o shortness of breath and palpitations. Unclear duration • Vitals per EMS: BP 110/71 mmHg, HR 140 bpm, RR 35 brpm, O2 sat 93% room air • The paramedics report crackles but no wheezing. They administered oxygen via facemask and brought her in. Meds are in the grocery bag CASE DETAILS AND INITIAL TRIAGE More BP=blood pressure; bpm=beats per minute; brpm=breaths per minute; c/o=complaining of;EMS= emergency medical services; HR=heart rate; O2 sat=oxygen saturation; RR=respiratory rate
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Vital Signs (in ER) • BP: 115/74 mmHg • HR: 141 bpm • RR: 33 brpm • Temperature: 37.3°C/99.2°F (oral) • O2 sat: 98% 2 L NC CASE DETAILS AND INITIAL TRIAGE BP=blood pressure; bpm=beats per minute; brpm=breaths per minute; ER=emergency room; HR=heart rate; NC=nasal cannula; O2 sat=oxygen saturation; RR=respiration rate
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • History of Present Illness • For the last 3 days, patient reports feeling increasingly short of breath, especially with exertion • She denies chest pain or pressure and denies any past h/o MI. She denies any history of HF • She does report sleeping on 2 extra pillows at night and that perhaps her shoes feel ‘tight’ • Only rest makes her feel better, though she feels her heart is ‘pounding’ CASE DETAILS AND INITIAL TRIAGE HPI More HF=heart failure; h/o=history of; MI=myocardial infarction
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Review of Systems • No: • cough or fever • black or bloody stools • nausea or vomiting • back, chest or abdominal pain • rash or hot/cold intolerance • Patient has: • fatigue • palpitations and shortness of breath CASE DETAILS AND INITIAL TRIAGE
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Past History • Past Medical History • Hypertension • Type II diabetes mellitus • Past Surgical History • Appendectomy • Cholecystectomy • Hysterectomy CASE DETAILS AND INITIAL TRIAGE More
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Allergy History, Medications, and Social History • Allergies • NKDA • Social History • No cigarettes • No illicit drugs • Alcohol only onweekends (6 pack) • Lives alone CASE DETAILS AND INITIAL TRIAGE • Current Medications • Hydrochlorothiazide 25 mg q.d. NKDA=no known drug allergy; q.d.=once daily
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Physical Examination (Focused Exam) • Appears in moderate distress • CV: tachycardic, irregular, “irregularly irregular”, no murmurs, gallops, rubs • (though it is loud in the ER and hard to hear) • Neck veins: + JVD • Lungs: rales 1/3 way up lung fields, no wheezing, equal and symmetric • Abdomen: Soft, not tender and not distended. No hepatomegaly • Skin: diaphoretic, 1+ pitting edema bilaterally, no calf tenderness • Some considerations… • Patient is short of breath with an irregularly irregular tachycardia • She has no past history of a dysrhythmia or heart failure or known coronary artery disease. However, absence of these does not rule them out • She has no fever, making pneumonia less likely. • There is no reported recent travel, h/o VTE, surgery, tobacco or hormone replacement therapy • There is no leg edema or swelling reported CASE DETAILS AND INITIAL TRIAGE CV=cardiovascular; ER=emergency room; h/o=history of; JVD=jugular venous distension; VTE=venous thromboembolism
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Click on the icons for more information Clinical Impression (Initial Diagnosis)and Differential Diagnosis Initial Plan of Care INITIAL DIAGNOSIS AND CARE PLAN Author: Peter S. Pang,MD, MS, FACEP, FAAEM FAHA, FACC
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Clinical Impression • New onset HF secondary to atrial fibrillation with rapid ventricular response • Other considerations: • Pneumonia • Pulmonary embolism • Acute coronary syndrome • Pericardial effusion/tamponade INITIAL DIAGNOSIS AND CARE PLAN HF=heart failure
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Initial Plan of Care • Treatment • i.v., O2, cardiac monitor, rhythm strip, ECG, portable CXR • Work-up • CBC, chem-7, Mg, troponin (not hs), BNP INITIAL DIAGNOSIS AND CARE PLAN BNP=B-type natriuretic peptide; CBC=complete blood count; CXR=chest X ray; ECG=electrocardiogram; hs=high sensitivity; i.v.=intravenous
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Initial Treatment • You order diltiazem 20 mg, slow i.v. push. However, you are concerned about the relatively long half-life and potential for systolic depression, especially if the patient has a reduced EF. Since she has no recent echo in her past history, you do a bedside US • You weren’t trained to determine EF and the patient is increasingly dyspneic lying flat. However, the heart has good function qualitatively • You go ahead with diltiazem 20 mg as well as furosemide 20 mg i.v. push INITIAL DIAGNOSIS AND CARE PLAN echo=echocardiogram; EF=ejection fraction; i.v.-intravenous; US=ultrasound
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Lab Results Click on the icons for more information ECG Chest X ray DIAGNOSTIC RESULTS Author: Peter S. Pang,MD, MS, FACEP, FAAEM FAHA, FACC
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • ECG(Rhythm Strip <5 min) • No clear p waves, irregular. Rate ~140-150 bpm DIAGNOSTIC RESULTS More bpm=beats per minute
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision ECG(<10 min from Arrival) DIAGNOSTIC RESULTS Click here for ECG: Interpretation ? QUESTION
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • ECG: interpretation • No clear p waves • Irregular rhythm • Narrow complex • Interpretation: AF with RVR DIAGNOSTIC RESULTS Click here for ECG: Interpretation AF=atrial fibrillation; RVR=rapid ventricular response
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Lab Results* (or Point of Care Testing Results) DIAGNOSTIC RESULTS • Click here for • Lab results:Reference Ranges • Na 133 mEq/L • K 4.6 mEq/L • BUN 24 mg/dL • Creatinine 1.1 mg/dL • Troponin I# 0.10 ng/mL (100 pg/mL) (elevated) • BNP ‡ 751 pg/mL (elevated) *Other labs are within normal reference ranges. #Abnormal Troponin I value >0.05 ng/mL, however NSTEMI criteria is >0.5 ng/mL. Abbott POC iStat assay. Reportable range 0.0 to 50.0 ng/mL. Upper 99% reference limit is 0.08 ng/mL. ‡Abbott POC iStat assay. Upper 95% reference range is 50 pg/mL. Reportable range is 15 to 5,000 pg/mL BUN=blood urea nitrogen; BNP=B-type natriuretic peptide; NSTEMI=Non ST-segment elevation myocardial infarction
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Chest X ray DIAGNOSTIC RESULTS Click here for Chest X ray: Interpretation
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Chest X ray: Radiology Interpretation • Mild cardiomegaly, cephalization, vascular congestion, interstitial edema, blunting of the left costal margin DIAGNOSTIC RESULTS
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Click on the icons for more information Revised Clinical Impression Next Actions REVISED DIAGNOSIS AND CARE PLAN Author: Peter S. Pang,MD, MS, FACEP, FAAEM FAHA, FACC
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Revised Clinical Impression • New onset AHF secondary to AF with RVR REVISED DIAGNOSIS AND CARE PLAN AF=atrial fibrillation; AHF=acute heart failure; RVR=rapid ventricular response
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Clinical Thinking… • Treatment • ECG demonstrates AF with RVR • Exam, lab work and CXR consistent with acute heart failure • Troponin is mildly elevated but does not meet NSTEMI threshold. In addition, ACS is less likely by history; though this remains on the differential • Infectious process might be obscured on CXR. However, no fever at this time REVISED DIAGNOSIS AND CARE PLAN ACS=acute coronary syndrome; AF=atrial fibrillation; CXR=chest X ray; ECG=electrocardiogram; NSTEMI= Non ST-segment elevation myocardial infarction; RVR=rapid ventricular response
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Patient Re-evaluation • HR has slowed after diltiazem to high 90 – low 100’s (bpm) • BP 121/86 mmHg • Patient has diuresed multiple times, but no exact I/O • Patient looks better and reports feeling better REVISED DIAGNOSIS AND CARE PLAN BP=blood pressure; HR=heart rate; I/O=input/output
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Next Steps (<3 hours) • Repeat ECG shows AF with HR in the high 90’s (bpm) • You order a diltiazem 5 mg/hr i.v. drip • You also order diltiazem 30 mg p.o. • You hold on further i.v. loop diuretic given brisk diuresis and plan to monitor frequently. • You consider anticoagulation. CHA2DS2-VASC score is 4 (moderate to high risk), counting her current AHF as history of HF. As you plan to admit the patient, you defer to the inpatient team REVISED DIAGNOSIS AND CARE PLAN AF=atrial fibrillation; AHF=acute heart failure; ECG=electrocardiogram; HF=heart failure; HR=heart rate; i.v.=intravenous; p.o.=by mouth
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Disposition • Admission to telemetry ward • As this is new onset AHF as well as new onset AF with RVR that was symptomatic, patient will require an in-depth evaluation for potential causes, as well as education for anti-coagulation and heart failure self-management • As patient reports palpitations, but the exact timing is unknown to the patient, assume >48 hours H DispositionDecision AF=atrial fibrillation; AHF=acute heart failure; RVR=rapid ventricular response
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision Click on the icons for more information Discussion and Conclusions Teaching Points Local Variation TEACHING POINTS, DISCUSSION AND CONCLUSIONS Author: Peter S. Pang,MD, MS, FACEP, FAAEM FAHA, FACC
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Teaching Points • Why not cardiovert? • In someone with HF, one could consider this an emergent indication for cardioversion. However, the patient is hemodynamically stable and duration of symptoms is unknown with certainty. This increases her risk for embolic stroke TEACHING POINTS, DISCUSSION AND CONCLUSIONS More HF=heart failure
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Teaching Points (Cont’d) • What about other drugs such as digoxin or -blocker to control her rate? • Neither would be absolutely contraindicated. Similar to non-dihydropyridine calcium channel blockers such as diltiazem, strong opinions may emerge re: choice of drug • There is no robust data on the pharmacological rate control management of AF with RVR and AHF in the ED setting • As this patient has presumed HFpEF, you chose diltiazem in part due to comfort and knowledge of the drug • If the patient had a reduced EF, digoxin or amiodarone would be more in line with guideline recommendations TEACHING POINTS, DISCUSSION AND CONCLUSIONS AF=atrial fibrillation; AHF=acute heart failure; ED=Emergency Department; EF=ejection fraction; HFpEF=heart failure preserved ejection fraction; RVR=rapid ventricular response
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Discussion and Conclusions • Patient has AF with RVR and new onset AHF. It is most likely that AF is the driver of the AHF. Managing the AF will improve the AHF symptomatology. However, AHF still requires treatment • Overall, the case is well managed. Whether or not to cardiovert depends on the history and duration of symptoms, with less stroke risk, the closer cardioversion occurs to the onset of symptoms (but always <48 hours per guidelines) • As new onset AHF, in general, patient should be admitted for further diagnostic and therapeutic management. In addition, education will be key for this patient with new diagnoses TEACHING POINTS, DISCUSSION AND CONCLUSIONS AF=atrial fibrillation; AHF=acute heart failure; RVR=rapid ventricular response
Home Revised Diagnosisand Care Plan Teaching PointsDiscussion and Conclusions CaseIntroduction Case Details and Initial Triage Initial Diagnosis and Care Plan DiagnosticResults DispositionDecision • Local Variation • Formal (as opposed to bedside point of care) echocardiography in the ED for new onset AHF or even decompensation, is uncommon TEACHING POINTS, DISCUSSION AND CONCLUSIONS AHF=acute heart failure; ED=Emergency Department
EHMRG Emergency Heart Failure Mortality Risk Grade. A tool that could be used to assess mortality risk at discharge. Note, this tool has not beenprospectively validated. Clinical judgement is important GP General practitioner. UK terminology.Theequivalent role in the US would be family physician R/O Ruled out Stat statim (Latin) referring to speed Specialist UK terminology. See consultant Acute Medicine Also known as emergency medicine ward CHA2DS2-VASC A clinical prediction rule for estimation of stroke risk in patients with atrial fibrillation CHEM7 US terminology. A basic metabolic panel including Na, K, Cl−,HCO3− or CO2, blood urea nitrogen, creatinine and glucose Community heart failure team UK terminology. A specialist community heart failure nursing service working in partnership with Hospital Trusts Consultant UK terminology. The equivalent role in the US would be an attending/staff physician C/O Complaining of
Lab results: Reference Ranges1,2 DIAGNOSTIC RESULTS • Blood gases, arterial (ambient air) pH 7.38–7.44 pCO2 35–45 mm Hg (4.7–6.0 kPa)pO2 80–100 mm Hg (10.6–13.3 kPa)O2 sat ≥95% • BNP, blood<100 pg/mL • BUN 8–20 mg/dL (2.9–7.1 mmol/L) • CRP 0.0–0.8 mg/dL (0.0–8.0 mg/L) • Ca, serum 9–10.5 mg/dL (2.2–2.6 mmol/L) Hematology • D-Dimer <500 μg/L (0.5 mg/L) • Hematocrit Male 41%–51% Female 36%–47% • Hemoglobin, blood Male 14–17 g/dL (140–170 g/L) Female 12–16 g/dL (120–160 g/L) • Platelets 150,000–350,000/µL (150–350 x 109/L) Blood, plasma and serum chemistry • Albumin, serum 3.5–5.5 g/dL (35–55 g/L) • ALT 0–35 units/L* • AST 0–35 units/L* More * Test performed at 37oC3 1. American College of Physicians, Laboratory Reference Values; 2. McMurray et al. Eur Heart J 2012:33;1787–1847; 3. http://www.surgeryencyclopedia.com/La-Pa/Liver-Function-Tests.html[accessed 20th February 2015]ALT=aminotransferase, alanine; AST=aminotransferase, aspartate; BNP=B-type natriuretic peptide; BUN=blood urea nitrogen; CRP=c-reactive protein
Lab results: Reference Ranges1,2 DIAGNOSTIC RESULTS • Urea nitrogen, blood 8–20 mg/dL (2.9–7.1 mmol/L) • Uric acid, serum 2.5–8 mg/dL (0.15–0.47 mmol/L) Urine • GFR, normal Male 130 mL/min/1.73 m2 Female 120 mL/min/1.73 m2 Blood, plasma and serum chemistry (cont’d) • Creatinine, serum 0.7–1.3 mg/dL(61.9–115 µmol/L) • Electrolytes, serumNa 136–145 meq/L (136–145 mmol/L)K 3.5–5.0 meq/L (3.5–5.0 mmol/L)Cl‾98–106 meq/L (98–106 mmol/L)HCO3 23–28 meq/L (23–28 mmol/L) • Glucose, plasma* 70–100 mg/dL (3.9–5.6 mmol/L) • Lactic acid, venous blood 6-16 mg/dL(0.67-1.8 mmol/L) 1. American College of Physicians, Laboratory Reference Values; 2. McMurray et al. Eur Heart J 2012:33;1787–1847GFR=glomerular filtration rate. *Fasting.