Download
1 / 1
10 likes | 172 Views
Severe Sepsis in Two Ugandan Hospitals: Management and Outcomes in a Predominantly HIV-1 Infected Patient Population. ST Jacob 1 , CC Moore 1 , P Banura 2 , R Pinkerton 1 , D Meya 3 , P Opendi 4 , SJ Reynolds 5 , N Kenya-Mugisha 6 , H Mayanja-Kizza 3 , and WM Scheld 1 , for the

E N D
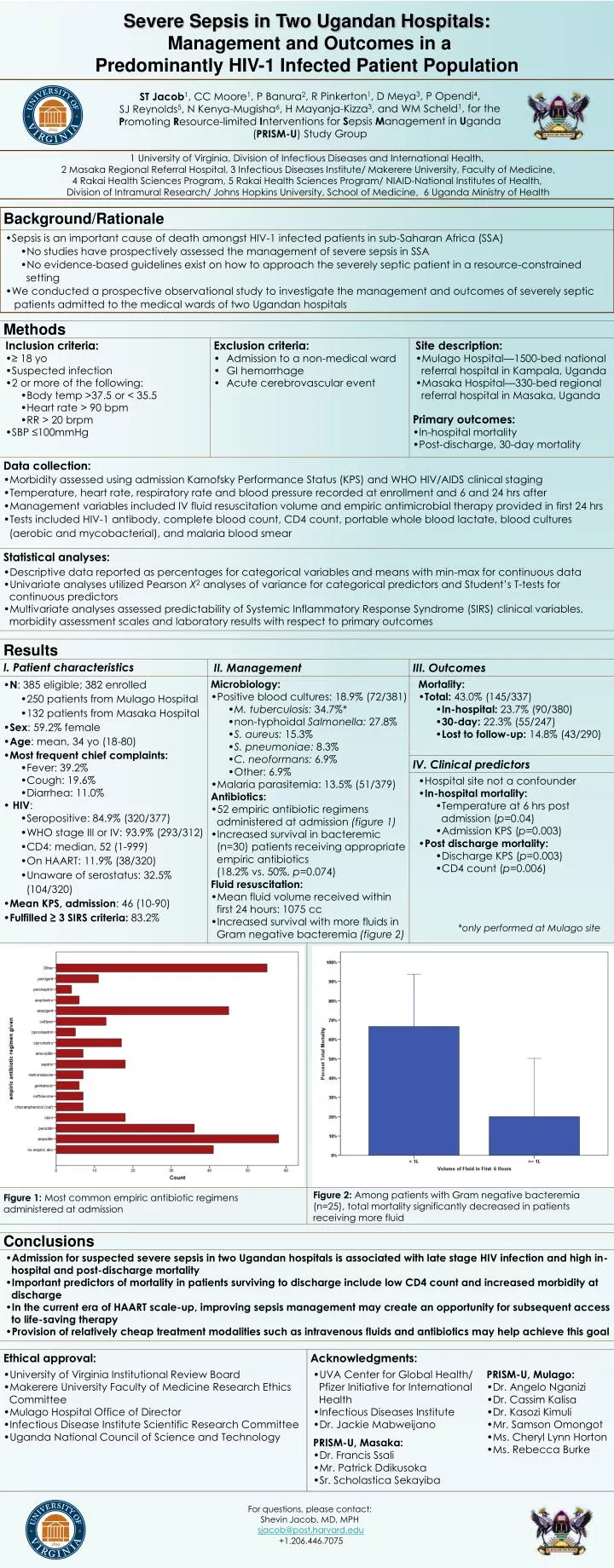
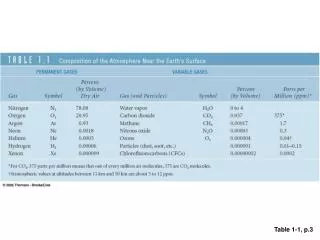
Severe Sepsis in Two Ugandan Hospitals: Management and Outcomes in a Predominantly HIV-1 Infected Patient Population ST Jacob1, CC Moore1, P Banura2, R Pinkerton1, D Meya3, P Opendi4, SJ Reynolds5, N Kenya-Mugisha6, H Mayanja-Kizza3, and WM Scheld1, for the Promoting Resource-limited Interventions for Sepsis Management in Uganda (PRISM-U) Study Group 1 University of Virginia, Division of Infectious Diseases and International Health, 2 Masaka Regional Referral Hospital, 3 Infectious Diseases Institute/ Makerere University, Faculty of Medicine, 4 Rakai Health Sciences Program, 5 Rakai Health Sciences Program/ NIAID-National Institutes of Health, Division of Intramural Research/ Johns Hopkins University, School of Medicine, 6 Uganda Ministry of Health Background/Rationale • Sepsis is an important cause of death amongst HIV-1 infected patients in sub-Saharan Africa (SSA) • No studies have prospectively assessed the management of severe sepsis in SSA • No evidence-based guidelines exist on how to approach the severely septic patient in a resource-constrained • setting • We conducted a prospective observational study to investigate the management and outcomes of severely septic • patients admitted to the medical wards of two Ugandan hospitals Methods • Inclusion criteria: • ≥ 18 yo • Suspected infection • 2 or more of the following: • Body temp >37.5 or < 35.5 • Heart rate > 90 bpm • RR > 20 brpm • SBP ≤100mmHg • Exclusion criteria: • Admission to a non-medical ward • GI hemorrhage • Acute cerebrovascular event • Site description: • Mulago Hospital—1500-bed national • referral hospital in Kampala, Uganda • Masaka Hospital—330-bed regional • referral hospital in Masaka, Uganda • Primary outcomes: • In-hospital mortality • Post-discharge, 30-day mortality Data collection: • Morbidity assessed using admission Karnofsky Performance Status (KPS) and WHO HIV/AIDS clinical staging • Temperature, heart rate, respiratory rate and blood pressure recorded at enrollment and 6 and 24 hrs after • Management variables included IV fluid resuscitation volume and empiric antimicrobial therapy provided in first 24 hrs • Tests included HIV-1 antibody, complete blood count, CD4 count, portable whole blood lactate, blood cultures • (aerobic and mycobacterial), and malaria blood smear Statistical analyses: • Descriptive data reported as percentages for categorical variables and means with min-max for continuous data • Univariate analyses utilized Pearson Χ2 analyses of variance for categorical predictors and Student’s T-tests for • continuous predictors • Multivariate analyses assessed predictability of Systemic Inflammatory Response Syndrome (SIRS) clinical variables, • morbidity assessment scales and laboratory results with respect to primary outcomes Results I. Patient characteristics II. Management III. Outcomes • N: 385 eligible; 382 enrolled • 250 patients from Mulago Hospital • 132 patients from Masaka Hospital • Sex: 59.2% female • Age: mean, 34 yo (18-80) • Most frequent chief complaints: • Fever: 39.2% • Cough: 19.6% • Diarrhea: 11.0% • HIV: • Seropositive: 84.9% (320/377) • WHO stage III or IV: 93.9% (293/312) • CD4: median, 52 (1-999) • On HAART: 11.9% (38/320) • Unaware of serostatus: 32.5% • (104/320) • Mean KPS, admission: 46 (10-90) • Fulfilled ≥ 3 SIRS criteria: 83.2% • Microbiology: • Positive blood cultures: 18.9% (72/381) • M. tuberculosis: 34.7%* • non-typhoidal Salmonella: 27.8% • S. aureus: 15.3% • S. pneumoniae: 8.3% • C. neoformans: 6.9% • Other: 6.9% • Malaria parasitemia:13.5% (51/379) • Antibiotics: • 52 empiric antibiotic regimens • administered at admission (figure 1) • Increased survival in bacteremic • (n=30) patients receiving appropriate • empiric antibiotics • (18.2% vs. 50%, p=0.074) • Fluid resuscitation: • Mean fluid volume received within • first 24 hours: 1075 cc • Increased survival with more fluids in • Gram negative bacteremia (figure 2) • Mortality: • Total: 43.0% (145/337) • In-hospital: 23.7% (90/380) • 30-day: 22.3% (55/247) • Lost to follow-up: 14.8% (43/290) IV. Clinical predictors • Hospital site not a confounder • In-hospital mortality: • Temperature at 6 hrs post • admission (p=0.04) • Admission KPS (p=0.003) • Post discharge mortality: • Discharge KPS (p=0.003) • CD4 count (p=0.006) *only performed at Mulago site Figure 2: Among patients with Gram negative bacteremia (n=25), total mortality significantly decreased in patients receiving more fluid Figure 1: Most common empiric antibiotic regimens administered at admission Conclusions • Admission for suspected severe sepsis in two Ugandan hospitals is associated with late stage HIV infection and high in- • hospital and post-discharge mortality • Important predictors of mortality in patients surviving to discharge include low CD4 count and increased morbidity at • discharge • In the current era of HAART scale-up, improving sepsis management may create an opportunity for subsequent access • to life-saving therapy • Provision of relatively cheap treatment modalities such as intravenous fluids and antibiotics may help achieve this goal Ethical approval: Acknowledgments: • University of Virginia Institutional Review Board • Makerere University Faculty of Medicine Research Ethics • Committee • Mulago Hospital Office of Director • Infectious Disease Institute Scientific Research Committee • Uganda National Council of Science and Technology • UVA Center for Global Health/ • Pfizer Initiative for International • Health • Infectious Diseases Institute • Dr. Jackie Mabweijano • PRISM-U, Mulago: • Dr. Angelo Nganizi • Dr. Cassim Kalisa • Dr. Kasozi Kimuli • Mr. Samson Omongot • Ms. Cheryl Lynn Horton • Ms. Rebecca Burke • PRISM-U, Masaka: • Dr. Francis Ssali • Mr. Patrick Ddikusoka • Sr. Scholastica Sekayiba For questions, please contact: Shevin Jacob, MD, MPH sjacob@post.harvard.edu +1.206.446.7075


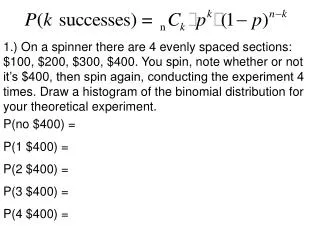
![1. 400 m 2. 200(1 + p ) m 3. 200[1 + ( p /2)] m 4. 200[1 + ( p /4)] m 5. zero](https://cdn3.slideserve.com/5442402/slide1-dt.jpg)
![A = p 4 B = p 5 CP = E[ p 7 , p 2 , p 3 , p 6 , p 1 , p 8 ] S[p 4 , p 5 ] d min = d 45](https://cdn3.slideserve.com/6420476/slide1-dt.jpg)