Download
1 / 87
870 likes | 1.06k Views
Strategies for Instructional Staff Working with Persons with Brain Injury and Vision Loss. B. J. LeJeune, CRC, CVRT Mississippi State University. Traumatic and Acquired Brain Injury. TBI . ABI.

E N D
Strategies for Instructional Staff Working with Persons with Brain Injury and Vision Loss B. J. LeJeune, CRC, CVRT Mississippi State University
Traumatic and Acquired Brain Injury TBI ABI Result of an organic, genetic or medical condition causing bleeding or lack of blood flow to the brain. Either permanently or temporarily alters functioning, thinking, processing and/or behavior May or may not respond to instructional interventions • Result of a blow, penetration or severe twist to the head and/or neck. • Either permanently or temporarily alters functioning, thinking, processing and/or behavior • May or may not respond to instructional interventions
Types of Primary Traumatic Brain Injuries • Diffuse Axonal Injury • Concussion (mildest and most common) • Contusion (bruising) • Coup-ContrecoupInjury (two part blow) • Second Impact Syndrome "Recurrent Traumatic Brain Injury“ • Skull Fracture • Penetration Injury • Shaken Baby Syndrome
Severity Measures of Brain Injury • Severity of insult to the brain • Length of time in coma • Deepness of coma • Functional physical and behavioral attributes • Area of the brain impacted may cause devastating effects of even a mild injury.
Glascow Coma Scale • Range of high of 15 to low of 3 • Higher the score the lower the degree of impairment. • Mild Injury – 13-15 • Moderate injury 9-12 • Severe – less than 8 • Motor response (1-6)+ eye opening (1-4)+ verbal response (1-5)
Severe Brain Injury Severity of Brain Injuries (Michigan Brain Injury Certification training program) Mild Brain Injury Loss of consciousness for less than 30 minutes Glasgow Coma Scale 13-15 Post Trauma amnesia of <24 hours Temporary or permanent altered mental or neurological state Post concussion symptoms Coma longer than 24 hours Glasgow Coma Score 3-8 Bruising/ bleeding in the brain Signs on EEG, CAT or MRI scans Long Term Impairments on one or more areas of life (i.e. home, work, community) Craniotomy - Surgical intervention • Loss of consciousness for more than 30 minutes, but less than 24 hours • Glasgow Coma Scale 8-12 • Possible Scull fractures with bruising/bleeding Signs on EEG, CAT or MRI scans • Some long term problems in one or more areas of life (i.e. home, work, community) Moderate Brain Injury
Major Brain Functions • Frontal Lobe- associated with reasoning, planning, speech, movement, emotions, personality, motivation, judgment, inhibition, and problem solving • Parietal Lobe- associated with sense of physical awareness, touch, movement, orientation, recognition, perception of stimuli
Major Brain Functions • Occipital Lobe- associated with visual processing • Temporal Lobe- associated with perception and recognition of auditory stimuli, memory, taste, smell, putting things into memory, interpretation of words, organization of time, and speech
Possible Impairments to the Right Side of the Brain • Visual-spatial impairment • Visual memory deficits • Left neglect (inattention to the left side of the body) • Decreased awareness of deficits • Altered creativity and music perception • Loss of “the big picture” type of thinking • Decreased control over left-sided body movements • Manic episodes
Possible Impairments Related to the Left Side of the Brain • Difficulties in understanding language (receptive language) • Difficulties in speaking or verbal output (expressive language) • Catastrophic emotional reactions (depression, anxiety) • Verbal memory deficits • Impaired logic • Sequencing difficulties • Depression • Decreased control over right-sided body movements
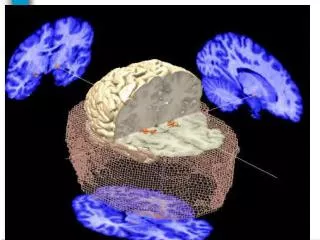
Vision and the Brain • Visual perception is a brain issue • The eye processes light and changes it to electronic impulses • The brain receives the impulses and changes them into an image • Visual understanding is a combination of the entry of light impulses to the brain and the brain’s ability to interpret those impulses.
Loss of Visual Field(Hemianopsia) • Loss of half-field of vision in each eye • Characterized by bumping into things, visually missing door jams, etc. • Left side causes difficulty reading or noticing things on the left.
Visual Neglect • Most frequently person will neglect certain visual positions – usually on the left • Different from field losses • Tend to veer to the left when walking • Bump into things in the neglect area
Left side Neglect Visual memory may be missing the neglected area
Visual Spatial Disorders • Depth perception issues • Personal Boundary Issues – body space issues • Eyes functioning differently both in terms of movement and focal points • Complexity issues • Difficulty locating obvious objects – Kite in clear sky…
Impaired Eye Movements • Saccadics (shifting gaze) Missing locations of items • Accommodative ability (inability to change focus) • Eye tracking (difficulty following movement) • Binocular abilities (Eye alignment/eye teaming) • Nystagmus – fairly common result of vision distruption from brain injury
Eye Strain, Brain Strain and Difficulty Reading • Eye strain can be related to dry eyes – caused by a number of things including lack of blink reflex • Confusion concerning content or recognizing words • Treatment: Frequent breaks, in some cases relearning reading, use of audio reading materials, artificial tears
Can you read this? fi uyoncaaredstih, uyovhea a sgtraennmdi too idcnuotllvbeieetath I lcudoaulacltyseudnatndrawth I saw dranige. The hpaonmnalewpero of the mhunanmdi, oaccdrgin to a srcheeahcr at mcabrigedmiuervtysi, it sden’totmaert in watheorrd the tlterse in a rwod are, the loynpiroamttnithgn is atth the rfsti and sltatltere be in htegrhticplea. htesrte can be a atoltsmes and oyu can islltarde it hwotuti a bpoerml. iths is cbuseea the uhanmnmidedosontraederveylteter by sitlfe, ubt the rwod as a lwoeh. Zanmig huh? yaeh and I walysatghuhtopslelign was ipmorattn!
Cna yuo raed tihs? fiyuocnaraedtihs, yuohvae a sgtranemnid too icdnuoltblveieetaht I cluodaulacltyuesdnatnrdwaht I was rdanieg. The phaonmnealpweor of the hmuanmnid, aoccdrnig to a rscheearch at CmabrigdeUinervtisy, it dseno'tmtaetr in wahtoerdr the ltteres in a wrod are, the olnyiproamtnttihng is taht the frsit and lsatltteer be in the rghitpclae. The rset can be a taotlmses and you can sitllraed it whotuit a pboerlm. Tihs is bcuseae the huamnmniddeos not raederveylteter by istlef, but the wrod as a wlohe. Azanmig huh? yaeh and I awlyastghuhotslpeling was ipmorantt!
Visual Hallucinations • Most frequent in the first year • Very real or awareness they are not real • Benign, threatening, traumatic • Charles Bonnet Syndrome
Light Sensitivity • Increased sensitivity to light • Causes headaches, pain, anxiety • Photophobia • Treatment: Filters (amber, violet, brown with UV & BV protection) • wide brimmed hat
Impaired Visual Memory • Inability to recognize faces, objects, letters • Concentration card game • Deficiencies are inclined to effect reading and spelling • Treatment: Developing • Memory Skills, Alternative strategies (50 First Dates)
Post Traumatic Vision Syndrome • Most common in children • blurred and double vision (lasts 6-12 months) • Can bring about the onset of vision related mannerisms (Blindisms)
Misquoting Somerset Maugham • “There are three rules to be effective in helping someone with a severe brain injury become totally restored, but unfortunately no one knows what they are.”
All Persons with Brain Injury are Different Older Persons who Fall Young People in Accidents
The Usual Continuum of Treatment for Moderate to Severe Brain Injuries • Intensive Care Unit • Trauma Unit in a Hospital • Rehabilitation Center for Brain Injuries • Home – In-Home Patient Care (OT, PT) • The Abyss or the do-it-myself Gap • Vocational Rehabilitation or Independent Living Services – Blind Services
All Brain Injuries are Serious • Mild Traumatic Brain Injury is a contradiction in Terms. All brain injury is Very Serious! • As the designation increases to moderate or severe the impact is even more devastating.
General Deficits in Moderate and Severe Brain Injuries • Memory Problems • Cognitive Disorders and Executive Function (problem solving, inhibition, initiation, etc.) • Time Management Difficulties • Social – Behavioral Issues • Difficulty with focus, multi-tasking, interruptions, distractions and visual complexity • Headaches, Tinnitis, motor difficulties • Depression and Corrupted Self-image
Assessment of the Individual: measuring the impact • Cognitive • Perception (Social, Time, etc.) • Memory (Abstract and Concrete, Short term and Long term) • Problem Solving (distractions, weighing options, focus, prioritizing) • Emotional • Behavioral/Social • Self Monitoring • Motor Functions • Vision
Vision Issues • Heminopsia • Double Vision • Loss of Recognition or visual memory • Visual Spatial Disorders • Visual Latency: Delay in interpreting what is seen • Convergence problems • Visual Fatigue, Dry Eyes, Nystagmus • Reading and writing disorders • Visual Neglect
Assessing the Network of Support • Assess the Individual and the Support Network • Critical to setting realistic and attainable goals • Issues such as: • Housing • Bill paying • Depression • Managing Medications • Self Awareness
Is the person ready for a Rehab Center for the Blind? • Traditional or Structured Discovery or a combination? • Medical Stability • Memory Issues • Sleep Issues • Motivation and goals • Medications • Social Skills & Behavioral Controls
Advantages of Center Based Rehab • Observation over time • Controlled environment • Noise and distractions • Food and drink • Class schedule • Support Network • Frequent reinforcement • Respite for family
Disadvantages of Rehab Center • Lack of family involvement • Forced Social Interactions • Need a flexible environment for rest breaks • May need a behavioral modification program – important to get appropriate protections and clearances • Unfamiliar environment • Protection from secondary falls
Things to consider…. Traditional Structured Discovery Independence goals may differ Accommodations to prevent falls under blindfold – balance issues. Memory issues can be complicated by lack of visual input. Rigor of class schedule may be too much – Longer stay - 12-24 months. Self-care issues – can a family member participate? • Length of stay will be longer • Are you going to work on therapeutically improving visual function? • Decisions about curriculum • Living issues – especially related to roommates. • Accommodating a family member
BI Rehabilitation Approaches Blind Rehab Approach BI Rehab Approach Start with the Support Network and try to slowly integrate independence Evaluate assistive technology and devices – sometimes as transitionary aids What can the person do themselves? What is their learning capacity? • What can the person do themselves? • What assistive technology might be useful? • When is it appropriate to have an aide to provide support – mostly in persons with additional needs…
Expanding the Team • Cognitive Therapist • Brain Injury Specialist • Speech Therapist trained in Cognition and Brain Injury • Assessment Team • Low Vision Services that understand cortical vision issues beyond Visual Acuity and Field Losses
Learning Prerequisites • Make sure the person is medically and behaviorally stable. • Evaluate if you can reason with the person. Are they aware of their limitations? Can they self-monitor? • Are there triggers that set them off? • Do they need another support person involved in process? Is there someone appropriate?
Brain Injury Rehab (www.headinjury.com/rehabcognitive.html) Brain injury rehabilitation involves two essential approaches: • Restoration of functions that can be restored – retraining the brain – neuroplasticity. • Learning alternative methods, how to do things differently when functions cannot be restored to pre-injury level.
Evidence-Based Practice • Evidence-based practice (EBP) "is the integration of best research evidence with clinical expertise and [consumer] values" (Sackett, Straus, Richardson, Rosenberg, & Haynes, 2000, p. 1). Clinical expertise refers to the use of practice skills and past experience to rapidly identify each [consumer's] unique circumstances and characteristics, "their individual risks and benefits of potential interventions, and their personal values and expectations" (p. 1).
Existing Teaching Literature • Majority of the literature is in brain injury only – does not include vision. • Veterans Affairs is the exception – they are beginning to publish. • Considerable BI information in both OT and SP literature. Meta Analyses and Experimental Studies which are good EBP. • Current trends are toward positive behavior supports and away from traditional instructional approaches.
Levels of Measurable Outcomes (WHO - ICF) • 1. Function Level: What can consumer see or perceive that s/he couldn’t see or perceive before? • 2. Activity: What can consumer do that s/he couldn’t do before? • 3. Participation: What does consumer do that s/he couldn’t do before? • 4. Quality of Life: What does consumer feel about what s/he can currently do?
Instructional Challenges: What do Job Coaches and Instructors need to know • What can the person learn? • What strategies will enhance learning? • Familiar settings • Situational instruction • At least daily, at time when the person is not fatigued. • As much as possible, include a significant other • Errorless Learning • Positive Supports • Brain Plasticity – In order to retrain the brain you must repeat, repeat, repeat. • Patience in the key for both the consumer and the instructor
Introducing Instruction • Take small steps at first and review frequently. • Tell them what you are going to teach – teach them - and tell them what they learned, then have them tell you what they learned. • Use the person’s name often – initially, and if they seem to be drifting or zoning. • Speak in a calm reassuring manner – but not talking down to the person. Pause frequently for the person to process what you have said. Don’t talk too fast. • Stress the importance of repetition and retraining the brain. Give homework.