Download
1 / 36
380 likes | 738 Views
ANTICOAGULANT. BY :DR ISRAA OMAR. Definition of Anticoagulation. Therapeutic interference ("blood-thinning") with the clotting mechanism of the blood to prevent or treat thrombosis and embolism. Indications of Anticoagulant Therapy. Treatment and Prevention of Deep Venous Thrombosis

E N D
ANTICOAGULANT BY :DR ISRAA OMAR
Definition of Anticoagulation • Therapeutic interference ("blood-thinning") with the clotting mechanism of the blood to prevent or treat thrombosis and embolism.
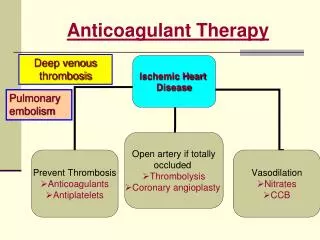
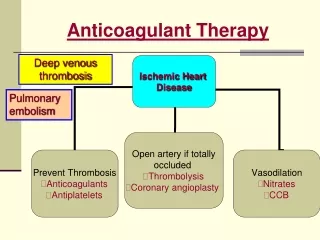
Indications of Anticoagulant Therapy • Treatment and Prevention of Deep Venous Thrombosis • Pulmonary Emboli • Prevention of stroke in patients with atrial fibrillation, artificial heart valves, cardiac thrombus. • During procedures such as cardiac catheterisation
Standard Heparin • Heterogeneous mixture of polysaccharide chains • MW 3k to 30k • Active in vitro and in vivo • Administration - parenteral- Do not inject IM - only IV or deep s.c. • Half-life 1 - 2 hrs - monitor APTT • Adverse effect - haemorrhage – • antidote - protamine sulphate
Heparin mechanism of action Heparin Antithrombin III Thrombin
Monitoring Heparin • Activated Partial Thromboplastin Time (APTT) • Normal range: 25-40 seconds • Therapeutic Range: 55-70 seconds
Low Molecular Weight Heparin • Changed management of venous thromboembolism • Standard (Unfractionated) heparin 30k • LMWH contains polysaccharide chains MW 5k • Enriched with short chains with higher anti-Xa:IIa ratio
Differences in Mechanism of Action • Any size of heparin chain can inhibit the action of factor Xa by binding to antithrombin (AT) • In contrast, in order to inactivate thrombin (IIa), the heparin molecule must be long enough to bind both antithrombin and thrombin • the chains of LMWH are not long enough to bind antithrombin and thrombin
Complications of Heparin • Hemorrhage(can be reversed by using protamine sulfate as an antidote) • Heparin-induced thrombocytopenia (HIT) and thrombosis • Osteoporosis (long-term only)more than 6 month ;the explanation of this side effect is unknown • Hyperkalemia • Hypersensitivity reaction
Heparin-Induced Thrombocytopaenia • Most significant adverse effect of heparin after haemorrhage • Most common drug-induced thrombocytopenia
Treatment of HIT • Discontinue all heparin • If need to continue anti-coagulation, use danaparoid (orgaran). • Avoid platelet transfusions • Thrombosis: use danaparoid or thrombin inhibitor(Hirudin)
Other Parenteral Anticoagulants DIRECT THROMBIN INHIBITORS Drugs • Lepirudin, desirudin, and bivalirudin, are modified forms of hirudin, the thrombin inhibitor present in the leech saliva. Mechanism of action • These drugs bind to the active site of thrombin so preventing its coagulant activity.
Adverse effects • Bleeding (no antidote is available) • Antibody formation (50% of patient receiving lepirudin): since the drug antibody complex retains anticoagulant activity, the duration of action can be increased. Therapeutic uses • As an alternative to heparin when heparin is contraindicated (patients at risk of heparin-induced thrombocytopenia, etc.).
Other Parenteral Anticoagulants Drotrecogin alpha The drug is a recombinant form of activated Protein C. Mechanism of action • Inhibition of coagulation by proteolytic inactivation of factor Vaand VIIIa.
Adverse effects • Bleeding (no antidote is available) Therapeutic uses • Given by IV infusion to patients with disseminate intravascular coagulation due to severe sepsis (the sepsis impairs the activation of protein C). • In this disease the drug leads to an absolute reduction of 6% in mortality.
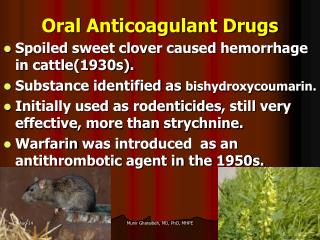
Oral anticoagulant • Warfarin is an oral anticoagulant that prevent thrombosis. Chemistry • Small, lipid soluble vit K analogs. • Warfarin is the only member of this group currently used in therapy.
Mechanism of action • Vitamin K is an essential cofactor for the synthesis of coagulation factors in the liver. • Vit K quinone is the active form. • Oxidation of this quinone to Vit K epoxide is coupled with carboxylation of coagulation factors II, VII, IX and X, as well as the anticoagulant factors proteins C and S. • Epoxide is then reconverted to quinone by Vitamin K epoxidereductase (VKOR). Warfarin blocks this reductive conversion and the carboxylation blockade results in incomplete molecules that are inactive in coagulation.
Vitamin K-Dependent Clotting Factors Vitamin K VII Synthesis of Functional Coagulation Factors IX X II
Warfarin Mechanism of Action Vitamin K Antagonism of Vitamin K VII Synthesis of Non Functional Coagulation Factors IX X II Warfarin
After Warfarin Administration • Warfarin action occurs only in vivo (in the liver) • Warfarin has no effect on the activity on the clotting factors that are already formed. • Therefore the onset of warfarin activity depends upon the rate of metabolism of these performed factors. • Their half lives are: • Factor II: 60 hrs • Factor VII: 8 hrs • Factor IX: 24 hrs • Factor X: 40 hrs • Protein C: 14 hrs
Therefore there is 3-5 day delay between the drug administration and the start of anticoagulant effect. • Transient protein C deficiency can also be induced because protein C and factor VII have the shortest half-lives of the coagulation factors. • Consequently protein C is inactivated whereas the intrinsic system remains active for a few days. This can cause transient hypercoagulability and local thrombosis.
Side effects of warfarin • Bleeding • Hepatotoxicity • Warfarin induced skin necrosis (can be reduced by starting heparin and warfarin concomitantly)
Warfarin: Major Adverse Effect—Haemorrhage • Factors that may influence bleeding risk: • Intensity of anticoagulation • Concomitant clinical disorders (liver disease ,thyrotoxicosis and fever ) • Concomitant use of other medications • Cimetidine and other enzyme inhibitors increase its action while rifampicin and other enzyme inducers inhibit the action of warfarin • aspirin increase its bleeding risk by working in synergistic fashion(PLATELETS INHIBITION) . • NSAIDS and chloral hydrate displace it from binding sites • Antibiotic eliminate the intestinal flora that produce vitamin k this will increase the risk of bleeding • Quality of management
Prothrombin Time (PT) • Historically, a most reliable and “relied upon” clinical test However: • Proliferation of thromboplastin reagents with widely varying sensitivities to reduced levels of vitamin K-dependent clotting factors has occurred • Problem addressed by use of INR (International Normalized Ratio)
Changing over from Heparin to Warfarin • May begin concomitantly with heparin therapy • Heparin should be continued for a minimum of four days • Time to peak antithrombotic effect of warfarin is delayed 96 hours (despite INR) • When INR reaches desired therapeutic range, discontinue heparin (after a minimum of four days)
Warfarin: Dosing & Monitoring • Start low • Initiate 5 mg daily • Educate patient • Stabilize • Titrate to appropriate INR • Monitor INR frequently (daily then weekly) • Adjust as necessary • Monitor INR regularly (every 1–4 weeks) and adjust
Contraindications to Warfarin Therapy • Pregnancy (it is a erotogenic drug can cause maxillofacial abnormality if given in the first trimester and increase the incidence of bleeding in the new born baby in the last trimester ;but it can be given in the middle trimester of pregnancy but with higher doses to achieve the target INR because there is hyper-coaguability state during pregnancy • Situations where the risk of hemorrhage is greater than the potential clinical benefits of therapy • Uncontrolled alcohol/drug abuse • Unsupervised dementia/psychosis
Signs of Warfarin Overdosage • Any unusual bleeding: • Blood in stools or urine • Excessive menstrual bleeding • Bruising • Excessive nose bleeds/bleeding gums • Persistent oozing from superficial injuries • Bleeding from tumor, ulcer, or other lesion
Reversing action of warfarin • Plasma (fresh frozen plasma or clotting factors) • Rapid but short-lasting, used mainly for life threating bleeding • Vitamin K • Not rapid, but lasts 1-2 weeks. Do not use if wishing to restart warfarin within next week. • In some cases only stopping the drug can be enough