Download
1 / 34
350 likes | 644 Views
The social context of health politics Health Politics. Ana Rico, Associate Professor Department of Health Management and Health Economics ana.rico@medisin.uio.no. O. Introduction The political system and the social systems I. Research question

E N D
The social context of health politicsHealth Politics Ana Rico, Associate Professor Department of Health Management and Health Economics ana.rico@medisin.uio.no
O. Introduction The political system and the social systems I. Research question Is the social context the main cause of policy? Does politics matter? II. Main concepts - definitions Context, social structure, power, politics, representation, national culture, convergence III. Thesis and arguments The social context directly determines policy We can treat politics as a black box IV. Aplications – Theories and evidence Structural theory: class and race National culture: Liberal (pro-market), non-Liberal (pro-state) Convergence theory: Pressures and policies OUTLINE: Theories of the social context
Context (= pressures external to the health care system) A subjective concept: variables in the background, which are assumed to be exogenous = independent from politics NOTE: There is wide agreement nowadays that most causal relationships in political science are endogenous Depending on the authors, the social context includes: A. Conjunctural factors: wars, crisis, etc.. B. International pressures: agreements, loans, competitors, multinationals C. Socioeconomic factors: income and social class, technology, demography, epidemiology D. Cultural factors: values, ideology, expectations WHAT IS THE SOCIAL CONTEXT? Mechanic, 1996. Comparative health systems
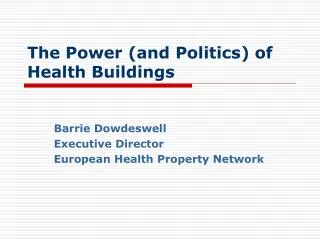
CAUSES OF POLICY CHANGE: Operationalization in WS/HC research • Access & participation • Policy strategies • Coalition-building • Competition and cooperat. • Changing resources • Learning • Conjunctural factors: ec crisis, wars • Socioeconomic structure: • Ownership, income • Education, knowledge • Social capital (status, support) CONTEXT • Sociopolitical structure: • Cleavages and political identities • Values: Culture and subcultures • Interest groups • Profesional assocs. • Poilitical parties • State authorities • Citizens: PO/SM • Mass media • Distrib. of formal pol. power: electoral law, constitution, federalism, corporatism • Contracts and org. structures • Norms of behaviour • Sanctions/incentives POLITICS: InteractionsProcess Preferences Resources POLITICAL ACTORS INSTITUTIONS Individual and collective - Formal and informal • Entitlements & rights • Regulation by law (of power, ownership, financing, behaviour, contracts) • Redistribution: Financing & RA • Production of goods & services POLICY Adapted from Walt and Wilson 1994
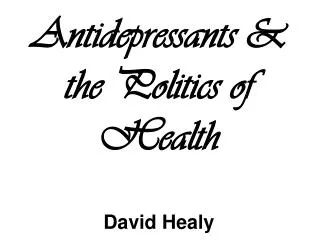
THE POLITICAL & SOCIAL SYSTEMS SOCIAL CONTEXT THE POLITICAL SYSTEM a Dynamic interactions Sociopolitical actors ECONOMY SOCIETY c Implemen- tation Policy change CULTURE b HC services Institutions Political actors Outputs d e f Outcomes POLITY POLITICS POLICY INPUTS OUTPUTS • Demands and supports • Access to the political system • Decision-making d. Institutional change e. Social impact of policy f. Distribution of costs and benefits
I. Research question Does the relative power of social groups determine policy? II. Main concepts - definitions Structure, cleavages, social groups, identities and ideological subcultures III. Thesis and arguments The distribution of ownership (+ other resources) across social groups determines their relative power to approve policies which favour them When priviledged groups have most resources, pro-rich policies prevail, and inequalities widen Underpriviledged groups will revolt (if they develop a political identity under capable leadership), in order to impose pro-poor policies When less ec. inequality + democracy, policy depends on the changing balance of power The distance between the middle class, and the rich/the poor, will determine who they support politically, and thus which policies will prevail V. Criticisms (antithesys and sinthesis) Social groups only influence policy via representatives (sociopolitical & political actors) + Powerful social groups can have weak representative organizations VI. Policy implications Redistribution of resources to less powerful social groups (or their representatives) is required to avoid conflict and for democracy to work OUTLINE (1): Structural theories
POWER RESOURCES:INFORMAL (social) & FORMAL (institutional) Collective action resources Knowledge-based resources • Informal, experience-based • Formal, evidence-based • Internal cohesion • Coalition capacity • External support Financial resources Institutional resources • Formal political power • Formal organizational power • Ownership • ”Sponsorship” Adapted from Hughes-Tuohy 2003 and Hicks & Mishra 1993
Policy MACRO: Political actors The political game MESO: Sociopol. actors $ HC SYSTEM Advisors and managers Political parties’ members Citizens’ Associations IGs - Bussiness - Insurance Profes. + providers’ Assoc. Patients’ Assoc. Patients’ Sociopol. context = Policy sub-system MICRO:Social actors The social context
Social structure, social groups and social power resources Social structure = Distribution of social power resources (ownership & income, knowledge & information, status & social support) across social groups Social groups are sets of individuals with shared characteristics (class, etnia, religion, community, gender) around which shared identities and subcultures are formed Some social groups develop conflicting ideological/political subcultures which tend to form opposition poles (cleavages or axis), usually associated to power resources imbalances WHAT IS THE SOCIAL STRUCTURE? Social groups Social structures, political institutions, social policies Political actors Individuals Organizations
Politics: Process through which political actors make, take and enforce collective decisions which committ all members of a society Power: 2 types Power for: As capacity to advance goals through intended action = capacity to decide among alternative courses of action Power over: As control upon. Capacity to obtain obedience (of conditioning others’ actions) even when it goes against self-interest Democratic representation: Relationship between political actors (representatives) and social groups (represented/constituency) by which group members delegate their decision rights in exchange for representatives’ committment to defend their interests and values in the political process with or without mandate: delegates versus representatives CONCEPTS
NOTE: Democratic politics requires representation CONCEPTS Decision costs Risk of despotism Number of decision-makers 100 Sartori, 1987
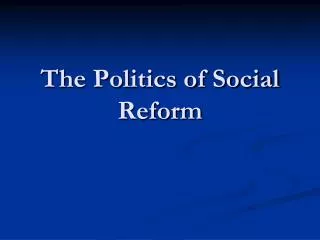
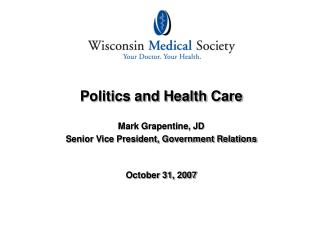
I. Research question Do national culture determine policy? II. Main concepts - definitions Culture, liberalism/statism III. Thesis and arguments Policies are only feasible if compatible with historical national cultures National cultures pre-date democracies, and do not change IV. Aplications – evidence Social expenditure in Anglosaxon countries vs. the rest V. Criticisms (antithesys and sinthesis) National culture is divided in ideological, conflicting subcultures National culture is the same as public opinion, and is directly influenced by politics (e.g. Persuasion, manipulation by political and social actors) National culture changes as a result of market/state performance (policy feedbacks) VI. Policy implications In Anglosaxon countries, only liberal welfare states can exist, in which state intervention is small, and relies on the market for provision of services NOTE: Initially, Esping-Andersen theory was a combination of structuralism and culturalism OUTLINE (2): Cultural theories
1. & 2.: THE WS, Measurement & Types Conservatism ITA AUS GER BEL FRA FIN IRE JAP NZ NETH NOR USA CAN UK DNK SWE AUZ SWI Neo-liberalism Socialdemocracy Based on Hicks & Kenworthy 2003
I. Research question Do countries converge towards same policies? II. Main concepts - definitions Context, globalization, convergence III. Thesis and arguments As pressures globalize, policies converge IV. Aplications – evidence Pressures and policies V. Criticisms (antithesys and sinthesis) Same pressures explain convergence, but not divergence Health care politics can account for both VI. Policy implications Convergence theory: An open economy, in the presence of international competition, guarantees adoption of best practice policies Political theory: Best practice will only be adopted if acceptable to political actors; compatible with previous institutions; and led by capable governments OUTLINE (3): Convergence theory
Convergence Defined as “the tendency of societies to grow more alike”, or as “The movement over time towards some identified common point” Note that: The essential theoretical emphasys is temporal, not spacial A “process of becoming”, not “a condition of being” Analytical dimensions of convergence: 1. Convergent pressures/social context 2. Convergent politics (=actors, institutions and process) 3. Convergent policies: Convergent policy goals Convergent policy content & instruments 4. Convergent outcomes Industrialization < modernization < globalization CONVERGENCE THEORY: RQs & CONCEPTS Bennett, 1992. What is policy convergence and what causes it?
Convergence led by industrialization & globalization: Industrialism:“As societies progressively adopt a progressively more industrial infrastructure, certain [automatic] processes are set in motion which tend overtime to shape social structures, political processes and public policies in the same mould” Globalized context pressures globalized economy convergent social structures, politics, policies and outcomes CONVERGENCE THEORY: THESIS & ARGUMENTS Bennett, 1992. What is policy convergence and what causes it?
Competition among countries and social darwinism Like in markets, most efficient innovations (best practice) spread automatically, without direct interaction Competition provides powerful incentives to converge in expenditure/imitate best practice Degree of adoption across countries depends on level openess of the economy to the international market The political system as a black box National politics do not have an impact in policy (as countries adopt the same policies independently of different national political and health care systems) CONVERGENCE THEORY: THESIS & ARGUMENTS Mechanic, 1996. Comparative health systems
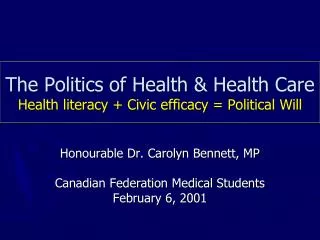
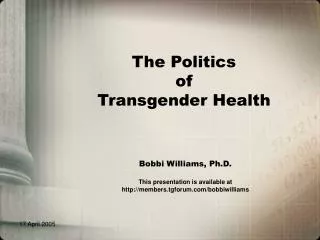
(1) PRESSURES A. Financial and macroeconomic pressures Slowly growing (or rapidly decreasing) GDP + Fiscal pressures to decrease taxes in order to boost exports and attract foreign investors B. Demographic and epidemiologic transition: Aging, through its effects on morbidity, (costs?) and financing Growing and changing inequalities C. Technology developments Solid evidence (OECD 2003) main cause of expansion in costs Important differences across countries on rate of investment D. Increased citizen expectations E. A widening and deepening EU NOTE: In political science, D & E are treated as endogenous to the political system, rather than exogenous/external factors. CONVERGENCE THEORY: APLICATIONS
Trends in total health expenditure as % of GDP, 1970 - 1999 12 Germany 10 France Sweden 8 Spain Percentage United Kingdom 6 4 2 0 1970 1975 1980 1985 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Year
Sweden Italy 18 EU average 17 16 15 14 CEE average 13 NIS average % of population aged 65+ 12 11 10 9 8 7 1970 1975 1980 1985 1990 1995 2000 Year TRENDS IN POPULATION AGED >65 BY EUROPEAN SUBREGIONS, 1970 - 1999 Source: WHO Health For All Database 2000
DIFFERENCE IN SMOKING PREVALENCE AMONG HIGH AND LOW STATUS GROUPS, 1995 (+ poor smoke more; - rich more)
(2) POLICIES 1. Cost-containment policies 2. From hierararchy to competition to cooperation 3. Transfer of autonomy to providers (power + risk) 4. Private management instruments 5. Regulated competition and cooperation 6. Expanding the role of patients 7. Transfer of financing responsibility - copayments 8. New rights and powers (eg choice) 9. Integrated care = coordination across levels of care 10. Strengthening of primary and community care 11. Promotion of new public health 12. Evaluation of performance CONVERGENCE THEORY: APLICATIONS
EVIDENCE ON THE CONVERGENCE THESIS Not enough research + evidence in health care (only on expenditure): Nixon (1999) and Hitris and Nixon on EU concludes YES suggests club convergence. General conclusion of a 1992 review (covering several policy sectors): “Although there is considerable evidence of policy convergence, which should convince us that it remains a significant topic for political sciencists, it is by no means a general finding. The literature provides plenty of evidence on divergent responses” (Bennett, 1992) Conclusions of a 2003 review on social expenditure and welfare policies: “The short term and middle term analysis show an spiralling link between the trend of social expenditure and economic development, and the existence of cycles... The cycle of social expenditure shows that a part of convergence is not due to any convergence in social policies...[but] The long-term convergent trend of social expenditure and its cycles have not blurred the distinction between the systems during the previous decades” (Bouget, 2003) CONVERGENCE THEORY: APLICATIONS
General criticisms from political science: “This [covergence] logic can easily collapse into an argument for economic or technological determinism” (Bennett, 1992) “Dominant groups in control of policy-making are able to impose an interpretation of context... which is not politically neutral” Pressures interact differently with diverse national institutions E.g. Aging (pressure) has very different impact on expenditure in a country with developed community care and health promotion; and with less investment in technology(eg Scandinavia vs. The US) The same policy ideas are applied through very different policy instruments E.g. Role of patients in financing US, Norway & Denmark (Mossialos et al, 2003) CONVERGENCE THEORY: V. CRITICISMS
IN SUM: There are nationally specific interactions between (shared) pressures and particular actor and institutional configurations There are some signs of converge but more of divergence Politics matters and can explain both convergence and divergence CONVERGENCE THEORY: SINTHESYS
CONVERGENCE THEORY: VI. POLICY IMPLICATIONS • Three positions on the dynamics of policy adoption across countries... • Two of them represent extremes: • All countries converge to a single model of best practice (ECONOMICS) • Each country develops its own policy models based on a trial and error process and on historical experiences, as policy problems differ across countries, and feasible policy solutions depend on nationally specific context, actors and institutions (INSTITUTIONALISM) • And the third, an intermediate position...: • Club convergence: there is a limited trend to convergence across nations with similar actor and institutional configurations which face similar context pressures (COMPARATIVE POLITICS)