Download
1 / 64
890 likes | 1.59k Views
Erectile Dysfunction in 2010. Erectile Dysfunction. Erectile dysfunction is defined as the consistent inability to attain or maintain a penile erection of sufficient quality to permit satisfactory sexual intercourse. The prevalence of this condition increases with age.

E N D
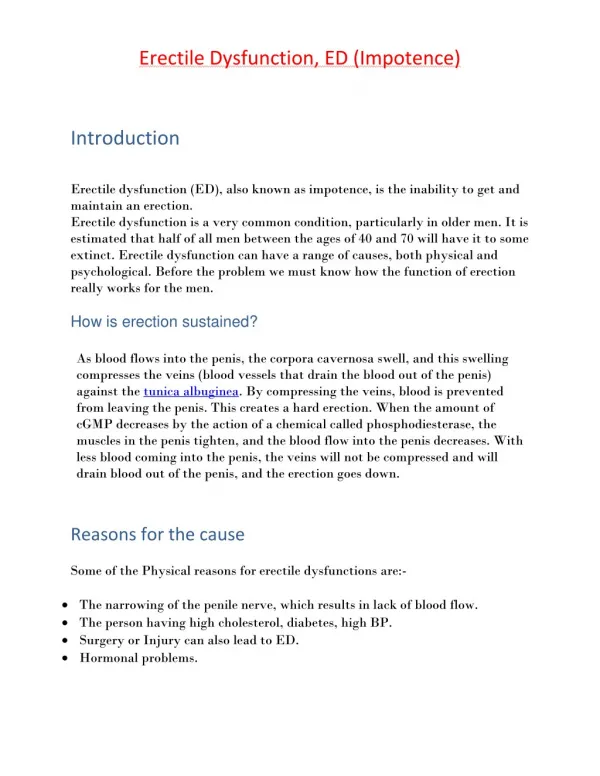
Erectile Dysfunction • Erectile dysfunction is defined as the consistent inability to attain or maintain a penile erection of sufficient quality to permit satisfactory sexual intercourse. • The prevalence of this condition increases with age. • It has been estimated that the worldwide prevalence of erectile dysfunction will be 322 million cases by the year 2025. • The risk of ED was 26 cases per 1000 men annually, which increased with age, lower education, DM, heart disease, and hypertension.
Moderate (25%) Minimal (17%) Erectile Dysfunction:Prevalence & SeverityMassachusetts Male Aging Study (MMAS)1 1709 men aged 40 to 70 years Complete (10%) Erectile dysfunction (52%) No erectile dysfunction (48%) 1. Feldman HA, et al. J Urol. 1994;151:54-61.
Common risk factors for ED • Atherosclerosis • Caused Vasculogenic ED, whereas endothelial damage is the proposed mechanism. • Aging • Alterations in the levels of NO that occur as a consequence of the aging endothelium. • Chronic illness, depression, and lack of a sexual partner are all prevalent in this aging population. • Chronic tobacco use • Caused vasculogenic ED because of its effects on the vascular endothelium. • Blood nicotine levels rise after smoking, which increases sympathetic tone in the penis and leads to nicotine-induced, smooth-muscle contraction in the cavernosal body. • leads to decreased penile NOS activity and neuronal NOS content.
Common risk factors for ED • Diabetes Mellitus • In the MMAS, the diabetic subset had a threefold increased prevalence of ED compared with nondiabetic subjects (28% versus 9.6%). • The overall incidence rate of ED was 26 cases per 1000 man-years in nondiabetics and 50 cases per 1000 man-years in the diabetic population. • The pathogenesis of ED in the diabetic patient is related to accelerated atherosclerosis, alterations in the corporal erectile tissue, and neuropathy. • Hypertension • Both antihypertensive agents as well as the disease itself also contribute to ED. • Certain classes of antihypertensive medications are notorious for their negative impact on erectile function, such as thiazides and β-blockers. • Hyperlipidemia • Contributed to ED by its relationship to endothelial dysfunction. • Study showed that decreasing total cholesterol to less than 200mg/dL by using atorvastatin (Lipitor) led to significant improvement of ED.
Clinical assessment of ED patients Differentiate between decreased libido and ED: assess whether the patient has one or both Tobacco use: type, amount, duration Alcohol intake History of depression or anxiety disorder Presence of social/relationship stressors Ability to have erections while masturbating versus when with partner List of all prescription, over-the-counter, and herbal medications Knowledge of whether nocturnal erections are present History of drug use: marijuana, cocaine, ketamine, other recreational drugs History of genitourinary trauma History of prostatic disease, or possible related symptoms History of hypertension, hyperlipidemia, CAD, peripheral vascular disease, cerebrovascular disease History of DM History of spinal cord injury History of penile plaques: possible Peyronie's disease Frequency of intercourse or attempted intercourse Ability to ejaculate
Tools for ED evaluation International Index of Erectile Function (IIEF) Sexual Encounter Profile (SEP) Global Assessment Question (GAQ)
International Index of Erectile Function (IIEF) a standardized questionnaire designed to measure ED and detect treatment-related changes reported by Rosen in 1997. It is a 15-item questionnaire addressing 5 different domains: erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction. The IIEF is the most frequently used efficacy measurement employed in ED drug trials. Using a scale from 1 (never/almost never) to 5 (almost always/always), men grade each domain. It is very sensitive and specific, and has been validated in 20 languages.
IIEF-5 To provide doctors with a “checklist” on erectile function that could be used in an office setting, an abridged 5-item version of the IIEF-15 has been developed by Rosen in 1999. 4 items are taken from the erectile function domain, plus another item addressing sexual intercourse satisfaction; it was chosen to reflect the central element in the NIH Consensus Panel (1992) definition of ED, which ties erectile function to satisfaction: “maintain erection of sufficient rigidity and duration to permit satisfactory sexual performance.” Perhaps the most important difference between the IIEF-15 and the IIEF-5 is that the latter asks patients to self-assess erectile function and satisfaction over the past 6 months, a more clinically relevant and practical time frame than 4 weeks. ED severity is classified into five categories based on the IIEF-5: severe (5 to 7), moderate (8 to 11), mild to moderate (12 to 16), mild (17 to 21), and no ED (22 to 25).
Sexual Encounter Profile (SEP) SEP is a five-question survey provided to patients with ED in clinical studies of oral therapies. The survey is completed after each sexual attempt. 1. Were you able to achieve at least some erection? 2. Were you able to insert your penis into your partner's vagina? 3. Did your erection last long enough to have successful intercourse? 4. Were you satisfied with the hardness of your erection? 5. Were you satisfied with the overall sexual experience? Answers to questions 2 and 3 are the ones most often used in the literature.
Global Assessment Questions (GAQ) GAQ is usually administered at the end of the treatment period during efficacy studies. Question 1: Has the treatment taken during the study improved your erections? Question 2: If yes, has the treatment improved your ability to engage in sexual activity? This is very subjective, and its responses tend to be valued less than SEP and IIEF.
In 2005, There Was the GBSS GBSS = Global Better Sex Survey October 2005 – March 2006 Authoritative global survey focusing on sexual aspirations and unmet needs of men and women 12,563 sexually active adults, aged 25-74 years 27 countries, including Australia,Japan, South Korea, Hong Kong Singapore, Taiwan, Indonesia, Malaysia, Thailand 5 Mulhall JP, et al. J Sex Med. 2008;5:788-795. Data on file – Pfizer Inc
GBSS The Next Step 2005 2008
AP SHOW Gather information on attitudes to sexual health, specifically for the Asia Pacific A diversity of cultural beliefs and practices Many people are uncomfortable talking about sexual health and many do not seek help Help people understand the importance of sexual health to overall health and wellbeing Encourage people to seek help for issues with sexual health The erection hardness scale (EHS) is used Asia Pacific Sexual Health and Overall Wellness (AP SHOW) 9
The EHS Provides a Clear Treatment Goal Towards Optimal Erection Hardness Suboptimal Erection Optimal Erection Severe ED Moderate ED Penis is hard enough for penetration but not completely hard Penis is hard but not hard enough for penetration Penis is larger but not hard Penis is completely hard and fully rigid Goldstein I, et al.N Engl J Med 1998;338:1397-1404. 11
Asia Pacific SHOW • 13 countries/regions • 3,957 sexually active men (2,016) and women (1,941) • Face-to-face interviews (self-completed questionnaire) / online self-administered method • May to July 2008 • The erection hardness scale (EHS) was used 12
Face-to-face or Internet Questionnaires 150 males and 150 females *subjects intercepted on street and handed a paper questionnaire to complete 13
Sex is very important % of people who indicate sex as very important in their lives
People very satisfied with sex % of people are very satisfied with sex in their lives
AP SHOW – Key Results In Hong Kong, 66% of men and 69% of women are not very satisfied with sex. Greater satisfaction with sex is strongly associated with greater satisfaction with other aspects of life. One in two men are not experiencing optimal erection hardness (EHS 4) during sexual activity. 60% of women report that their partners do not have optimal erection hardness (EHS 4) during sexual activity. Men with and women whose partners have optimal erection hardness (EHS 4) are more satisfied with sex than men with and women whose partners have suboptimal erection hardness (EHS 3). Men with suboptimal erection hardness (EHS 3) report they have less sex than they should, and are less satisfied with sex and other aspects of the sexual experience than men with optimal erection hardness (EHS 4). 15
1 In Hong Kong, 66% of men and 69% of women are not very satisfied with sex. Greater satisfaction with sex is strongly associated with greater satisfaction with other aspects of life. 16
Many Men and Women Are Not Very Satisfied with Sex • Overall, 66% of men and 69% of women are not very satisfied with sex 69% 66% 25% VERY SATISFIED 22% 13% COMPLETELY SATISFIED 6% MEN WOMEN 19
More than satisfied with sex 0-19% 60-93% MEN WOMEN Those More Satisfied with Sex Are More Satisfied with Top Priorities in Life Less than satisfied with sex Satisfied with: Being a spouse/partner Family life Being a parent Overall physical health Financial well-being Men: 1) Being a spouse/partner; 2)Family life; 3) Overall Physical health; 4) Financial well-being ; 5) Being a parent Women: 1) Overall Physical health; 2) Being a spouse/partner; 3) Family life and being a parent; 5) Financial well-being 21
2 One in two men are not experiencing optimal erection hardness (EHS 4) during sexual activity. 60% of women report that their partners do not have optimal erection hardness (EHS 4) during sexual activity. 20
3 Men with and women whose partners have optimal erection hardness (EHS 4) are more satisfied with sex than men with and women whose partners have suboptimal erection hardness (EHS 3) 22
Erectile hardness and Satisfaction with sex MEN WOMEN 22% vs. 38%
4 Men with suboptimal erection hardness (EHS 3) report they have less sex than they should, and are less satisfied with sex and other aspects of the sexual experience than men with optimal erection hardness (EHS 4) 25