Download
1 / 38
400 likes | 858 Views
HKCEM College Tutorial. Cervical spine injury & Trauma Score . Author Dr. Au Yeung Kwan Leong August, 2013. Case presentation. M/65, Taxi driver PMH: HT, IHD Assaulted by passenger Being pushed onto ground and landed on back Pre-hospital vitals: BP= 160/92 P= 81 AV P U

E N D
HKCEM College Tutorial Cervical spine injury & Trauma Score Author Dr. Au Yeung Kwan Leong August, 2013
Case presentation • M/65, Taxi driver • PMH: HT, IHD • Assaulted by passenger • Being pushed onto ground and landed on back • Pre-hospital vitals: • BP= 160/92 P= 81 • AVPU • What should be applied to this patient at scene?
Spine board • Cervical collar • +/- Oxygen supplement
On arrival to A&E • BP= 110/66 P= 71 • SaO2 99% room air • E3V4M1 • Not cooperative during physical examination • Primary & secondary survey • Unremarkable • Trauma series
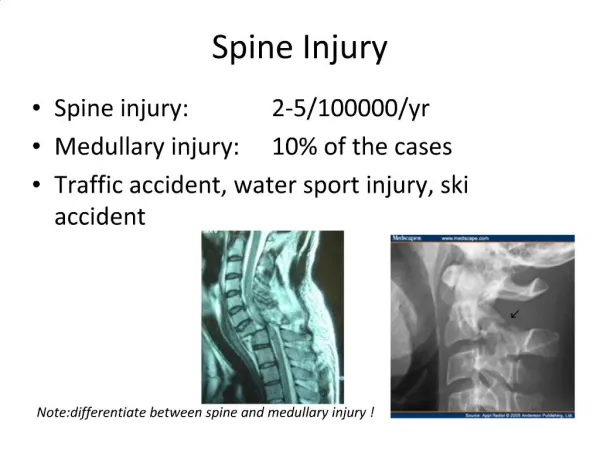
X-Ray C-spine XR comment?
XR c-spine • C1-5 shown • Loss of lordosis • No fracture seen • CXR, Pelvic XR unremarkable • FAST scan: no free fluid
What are the essential investigations for a trauma patient with impaired conscious level?
Disposal • In view of unremarkable physical and imaging results, and abnormal ECG, the patient was admitted to medical ward for further investigation of the impaired conscious level. • Neck collar and spine board were taken off. • Is it the appropriate time?
Medical ward (Day 1) • Conscious level improved after admission • Neurological exam showed • Conscious + oriented • Limb power ~4/5 ?limited by muscle pain • Noted TnI (2.99), CK (4280), ECG TWI V1-5 Impression: ACS started aspirin, enoxaparin
Day 2 after admission • c/o sudden onset of neck pain with 4 limb weakness + sensation • Urgent consulted Orthopaedic Surgeon
XR c-spine was repeated • What level of c-spine should be included to say a c-spine XR is adequate? • What are the methods to improve the adequacy of a c-spine XR?
Swimmer's view (taken with one arm extended over the head) • Repeat XR with the cervical collar removed • Traction on arms if no arm injury is present (pull shoulders) ! May cause further damage in patients with suspected neck injury
What do you suspect? What next?
Unilateral vs Bilateral Facet joint dislocation Unilateral Locked Facet Bilateral Facet Dislocation Severe flexion injury Both anterior and posterior ligamentous structures are disrupted at site of injury More superior vertebra subluxes forward by 50% or more of the body below Usually occurs in lower cervical spine 85% neurologic deficits • Flexion/distraction and rotation injury • Inferior articular facet of superior vertebral body is locked in front of the superior facet of the inferior vertebral body on one side • Slight anterior subluxation of one vertebral body on the one below, Usually less than 25% of the width • Spinous processes do not align on frontal film • displaced toward the locked side • Most often occurs at C4-5 and C5-6 • 30% associated with neurologic defect
MRI C-spine Comment?
Day 3 progress • Urgent MRI C- & T-spine: Right C5/6 facet dislocation and left C5/6 facet subluxation with spinal cord compression and edema. • IV methylprednisolone was given • Transferred to O&T ward • Not for emergency surgery for SCI in view of ACS • Halo-ring applied
Progressive downhill course Patient developed Chest infection with MRSA cultured in Sputum Vancomycin & Levofloxacin, Fusidic acid Type II resp failure intubated and mechanically ventilated Bradycardia and shock inotropes Finally succumbed and certified dead on day 28
Postmortem Findings • Spine • Callus formation at right C5 facet joint with surrounding soft tissue torn, haematoma track down along fascia to thoracic level • Local edema along C3-7 spinal cord, neuron loss with inflammatory changes • No epidural/ subdural haematoma found • Dislocation well restored • Brain • Right temporal lobe liquefactive necrosis ?CVA • No associated feature of traumatic brain injury • Heart • Coronary artery disease ( >90% stenosis) • Ischaemic changes • Lungs: • Edema and consolidation worse at RLL
ISS= 17 RTS= 4.0936 Probability of Survival (PS)= 0.4249 What do these number means?
Cervical spine injury • The spinal cord injury occurs • at the time of trauma in 85% of patients and • as a late complication in 15%. • The initial postinjury period is critical with regard to neurologic recovery or deterioration. • Delayed recognition of an injury or improper stabilization of the cervical spine may lead to irreversible spinal cord injury and permanent neurologic damage.
Stability • A spinal injury is stable when controlled movements will not cause a neurological deficit. • For an unstable injury, controlled movements can lead to or aggravate neurological damage.
Denis’ 3 Column Classification • Anterior column : ALL, anterior half of vertebral body, anterior part of annulus fibrosus • middle column : posterior half of vertebral body, PLL, posterior part of annulus fibrosus • posterior column : neural arch, ligamentumflavum, facet joint capsules, interspinous and supraspinous ligaments Our patient has at least 2 column injuries.
If any two of these 3 columns are disrupted, the spine is rendered unstable.
The NEXUS Low-Risk Criteria C-spine imaging is recommended for patients with trauma unless they meet all of the following criteria: • Absence of posterior midline cervical-spine tenderness # • No evidence of intoxication, • A normal level of alertness and consciousness (baseline mental status) • Absence of focal neurological deficit • Absence of any distracting injuries
CT scan of C-spine • Most injuries can be diagnosed by plain films; but up to 20 % of fractures are missed on conventional radiographs • If there is a question on the radiograph, CT of the cervical spine should be obtained. • Particularly useful in fractures that result in neurologic deficit and in fractures of the posterior elements of the cervical canal (e.g. Jefferson's fracture)
MRI of C-spine • MRI is indicated in cervical fractures that have • spinal canal involvement, • clinical neurologic deficits or • ligamentous injuries. • MRI provides the best visualization of the soft tissues • ligaments, intervertebral disks, spinal cord, and epidural hematomas.
Trauma score • More than 50 scoring systems have been published for the classification of trauma patients in the field, emergency room, and intensive care settings. • Trauma scoring systems convert the severity of an injury into a number, facilitating • Interpretation of trauma literature • Decipher operative reports • Comprehend methods of predicting patient outcome
Three main groups of trauma scores: • Anatomical • Abbreviated injury scale (AIS) • Injury severity score (ISS) • New injury severity score (NISS) • Anatomic profile (AP) • Physiological • Revised trauma score (RTS) • Glasgow coma score (GCS) • Acute physiology and chronic health evaluation (APACHE) • Combined • Trauma and Injury severity score (TRISS) • International classification of diseases-based ISS (ICISS)
Revised Trauma Score (RTS) • physiological scoring system • high inter-rater reliability • high accuracy in predicting death • scored from the first set of data obtained on the patient, and consists of • Glasgow Coma Scale, Systolic Blood Pressure and Respiratory Rate. • RTS = 0.9368 GCS + 0.7326 SBP + 0.2908 RR
: The RTS correlates well with the probability of survival
Injury Severity Score (ISS) • Anatomical scoring system • provides an overall score for patients with multiple injuries. • Each injury is assigned an Abbreviated Injury Scale (AIS) score and is allocated to one of six body regions • (Head, Face, Chest, Abdomen, Extremities (including Pelvis), External) • Only the highest AIS score in each body region is used. • The 3 most severely injured body regions have their score squared and added together to produce the ISS score.
Trauma Score- Injury Severity Score (TRISS) • Determines the probability of survival (Ps) of a patient from the ISS and RTS using the following formulae: • The coefficients b0 - b3 are derived from multiple regression analysis of the Major Trauma Outcome Study (MTOS) database. AgeIndex is 0 if the patient is below 54 years of age or 1 if 55 years and over. b0 to b3 are coefficients which are different for blunt and penetrating trauma. If the patient is less than 15, the blunt coefficients are used regardless of mechanism.
Summary • Evaluation of the neck injury in trauma patients • Clinical • X-ray • CT scan • MRI • Different types of Trauma score