Download
1 / 13
170 likes | 644 Views
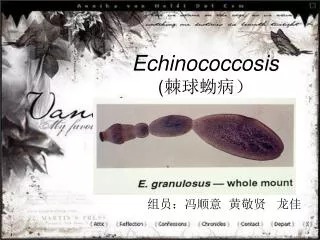
Echinococcosis. Aswad H. Al.Obeidy FICMS, FICMS GE&Hep Kirkuk General Hospital. Echinococcosis. Larval stage of the Echinococcus granulosus complex, E. multilocularis , E. oligarthrus or E. vogeli . E. granulosus complex Produce unilocular cystic lesions

E N D
Echinococcosis Aswad H. Al.Obeidy FICMS, FICMS GE&Hep Kirkuk General Hospital
Echinococcosis • Larval stage of the Echinococcus granulosus complex, E. multilocularis, E. oligarthrus or E. vogeli. • E. granulosus complex Produce unilocular cystic lesions • Are prevalent in areas where livestock is raised in association with dogs • High prevalence in China, central Asia, the Middle East, the Mediterranean region, eastern Africa, and parts of South America • E. granulosus strains may actually belong to more than one species; specifically, strains from sheep, cattle, pigs, horses, and camels probably represent separate species • E. multilocularis, which causes multilocular alveolar lesions that are locally invasive, is found Canada, the United States, central and northern Europe; China; and central Asia • E. vogeli causes polycystic hydatid disease and is found only in Central and South America • Cysts develop in the intermediate hosts
Etiology • The adult E. granulosus worm is small (5-mm-long) • Lives for 5–20 months in the jejunum of dogs • The adult Echinococcus tapeworm consists of a scolex, which contains a rostellum with 20 to 50 hooklets and 4 suckers, a neck, and an immature, mature, and gravid proglottid • The gravid segment splits to release eggs that are morphologically similar to Taenia eggs and are extremely hardy • Embryos escape from the eggs, penetrate the intestinal mucosa, enter the portal circulation, and are carried to various organs, most commonly the liver and lungs • Daughter cysts develop from the inner aspect of the germinal layer, as do germinating cystic structures called brood capsules • New larvae, called protoscolices, develop in large numbers within the brood capsule • The cyst wall contains three layers: an outer adventitial layer, which is host-derived and can calcify, and an intermediate acellular layer and inner germinal layer, which are worm-derived • Cysts typically increase in diameter at a rate of one to five centimeters per year • 85 to 90 percent of patients with E. granulosus have single-organ and more than 70 percent have only one cyst
Clinical Manifestations • Asymptomatic until their expanding size or their space-occupying effect in an involved organ elicits symptoms • Latent periods of more than 50 years before symptoms reported • The liver (70%)The right lobe in 60 to 85 % and the lungs(20%) Followed by the kidney, spleen, brain, and bone • May be discovered incidentally on a routine x-ray or ultrasound study • Hepatic echinococcosis who are symptomatic most often present with abdominal pain or a palpable mass in the right upper quadrant • Compression of a bile duct or leakage of cyst fluid into the biliary tree may mimic recurrent cholelithiasis, and biliary obstruction • Ruptureof or episodic leakage from a hydatid cyst may produce fever, pruritus, urticaria, eosinophilia, or anaphylaxis • Pulmonary hydatid cysts may rupture into the bronchial tree or peritoneal cavity and produce cough, dyspnea, chest pain, or hemoptysis • Other presentations are due to the involvement of bone (invasion of the medullary cavity with slow bone erosion producing pathologic fractures), the CNS (space-occupying lesions), theheart(conduction defects, pericarditis), and the pelvis (pelvic mass) • Rare complications of hydatid cysts or cyst rupture include pancreatitis, portal hypertension, and rupture into the pericardial sac
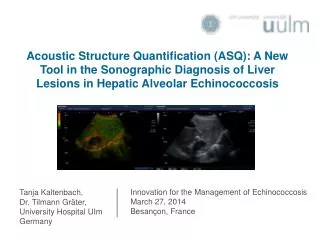
Diagnosis • Plain films will define pulmonary cysts of E. granulosus—usually as rounded masses of uniform density • MRI, CT, and ultrasound as well-defined cysts with thick or thin walls • When older cysts contain a layer of hydatid sand that is rich in accumulated protoscolices, these imaging methods may detect this fluid layer of different density • The most pathognomonicfinding, if demonstrable, is that of daughter cysts within the larger cyst • This finding, like eggshell or mural calcification on CT, is indicative of E. granulosus infection and helps to distinguish the cyst from carcinomas, bacterial or amebic liver abscesses, or hemangiomas • A specific diagnosis of E. granulosus infection can be made by the examination of aspirated fluids for protoscolices or hooklets • Serodiagnostic assays can be useful, although a negative test does not exclude the diagnosis of echinococcosis. Cysts in the liver elicit positive antibody responses in ~90% of cases, whereas up to 50% of individuals with cysts in the lungs are seronegative • Antigen 5 and antigen B are the two major antigens of E. granulosus utilized in serologic testing • An ELISA or indirect hemagglutination assay also may be used for diagnosis, with sensitivity rates of 90% • Detection of antibody to specific echinococcal antigens by immunoblotting has the highest degree of specificity
Ultrasound staging • The ultrasound appearance includes lesions classified as active, transitional, and inactive • Active cysts include types CL (with a cystic lesion and no visible cyst wall), CE1 [with a visible cyst wall and internal echoes (snowflake sign)], and CE2 (with a visible cyst wall and internal septation). • Transitional cysts (CE3) may have detached laminar membranes or may be partially collapsed • Inactive cysts include types CE4 (a nonhomogeneous mass) and CE5 (a cyst with a thick calcified wall)
Gharbi classification • Divides cysts into five types • Type I cysts consist of pure fluid • Type II have a fluid collection with a split wall • Type III cysts contain daughter cysts (with or without degenerated solid material) • Type IV have a heterogeneous echo pattern • Type V have a calcified wall
Treatment • Surgery has traditionally been the principal definitive method of treatment. • The overall cure rate for surgery is approximately 90 percent • Surgical mortality is usually 0.5 to 4 percent for the first intervention • For CE1 lesions, uncomplicated CE3 lesions, and some CE2 lesions, PAIR (percutaneous aspiration, infusion of scolicidal agents, and reaspiration) is now recommended instead of surgery • PAIR is contraindicated for superficially located cysts (because of the risk of rupture), for cysts with multiple thick internal septal divisions (honeycombing pattern), and for cysts communic. with the biliary tree • For prophylaxis of secondary peritoneal echinococcosis due to inadvertent spillage of fluid during PAIR, the administration of albendazole (15 mg/kg daily in two divided doses) should be initiated at least 4 days before the procedure and continued for at least 4 weeks afterward • After aspiration, contrast material should be injected to detect occult communications with the biliary tract. Alternatively, the fluid should be checked for bile staining by dipstick • Daughter cysts within the primary cyst to be punctured separately • This approach yields rates of cure and relapse equivalent to those following surgery
Treatment • Surgery remains the treatment of choice for complicated E. granulosus cysts (e.g., those communicating with the biliary tract) or for areas where PAIR is not possible • The preferred surgical approach is pericystectomy, in which the entire cyst and the surrounding fibrous tissue are removed • The risks posed by leakage of fluid during surgery or PAIR include anaphylaxis and dissemination of infectious protoscolices • Minimized by careful attention to the prevention of spillage of the cyst and by soaking of the drapes with hypertonic saline • Infusion of scolicidal agents is no longer recommended because of problems with hypernatremia, intoxication, or sclerosing cholangitis • Albendazole, which is active against Echinococcus, should be administered adjunctively, beginning several days before resection and continuing for several weeks for E. granulosus • Praziquantel (50 mg/kg daily for 2 weeks) may hasten the death of the protoscolices • Medical therapy with albendazole alone for 12 weeks to 6 months results in cure in ~30% of cases and in improvement in another 50%
Complications • Infection of the residual cavity • Intraabdominal abscesses • Anaphylactic reactions • Spillage of parasite material leading to secondary echinococcosis • Biliary fistulation • Sclerosing cholangitis
Contraindications • According to the World Health Organization (WHO) recommendations, surgery is contraindicated in: • Patients whose general condition is very poor • Patients at the extremes of age • Pregnant women • Patients with multiple cysts or cysts that are difficult to access • Patients with dead or totally calcified cysts
Medical therapy • WHO recommendations state that medical therapy should be used for • Patients with inoperable disease or those unfit for surgery • Patients with multiple cysts in two or more organs • Multiple small liver cysts or cysts deep in liver parenchyma • Peritoneal cysts • Patients following incomplete surgery or relapse • Prevention of secondary spread of echinococcal infection following spontaneous rupture or aspiration of cysts
Prevention • Administering praziquantel to infected dogs • Denying dogs access to infected animals • Vaccinating sheep • Limitation of the number of stray dogs