Download

1 / 46
460 likes | 536 Views
HHR Chair, OHHRRN & CHHRN . Dr. Ivy Lynn Bourgeault October 28 2011. Presentation for HealthGOv , Sydney. CIHR/Health Canada Chair in Health Human Resource Policy. Dr. Ivy Lynn Bourgeault March 31/11. Overview. Background to Chair in Health Human Resource Policy

E N D
HHR Chair, OHHRRN & CHHRN Dr. Ivy Lynn Bourgeault October 28 2011 • Presentation for HealthGOv, Sydney
CIHR/Health Canada Chair in Health Human Resource Policy Dr. Ivy Lynn Bourgeault March 31/11
Overview • Background to Chair in Health Human Resource Policy • Previous/Ongoing Studies related to HHR • HHR Chair Research Program • Capacity enhancement • Community linkages • OHHRRN ... CHHRN
What is HHR? • At its most basic component, this area of research answers the questions of who should do what where and how in the provision of care. • It typically addresses the human resources needed within a health care system. • Often neglected in this research are the human resources for health care that are provided more informally. • More recently, and perhaps in more international audiences, the term is referred to as human resources for health – which as the term suggests focuses more broadly on the human resources necessary to improve the health of a population.
Why study HHR? • It is perplexing how the health care system costs us billions of dollars yet there is very little research or indication of evidence-based policy decision-making about who should be delivering care in this billion dollar system and how they should be going about doing it. • It is even more perplexing that we tend to solve some of the persistent problems in the delivery of health care in Canada – particularly the shortages in rural and remote locations – by creating even more critical crises in other countries? • It is pretty astounding to be made aware of the statistic that over 1 billion people in the world have not and will never have access to health worker. http://www.healthworkermigration.com/videos/226-health-workforce-alliance.html • These are some of the reasons why I study health human resources policy.
Context of HHR Research in Canada • Goal: • effective approaches to the planning, management and training of HHR that meets the population's needs today and in the future. • Problem: • HHR planning is complex, multifaceted and influenced by a wide variety of exogenous as well as endogenous factors to health care systems which vary across time.
Context of HHR Research in Canada • HHR Literature: • Largely quantitative and focused on modeling and projections • History of getting it wrong, largely because the complexity is not fully appreciated • e.g., IMGs solving Rural shortages
CIHR/Health Canada HHR Chair Program TITLE OF MY APPLICATION • Unpacking the Contextual Influences on Health Human Resources through Comparative Research and Conceptual Modeling • The primary objective of this research chair will be to further expand upon our initial model through the conduct of targeted comparative research.
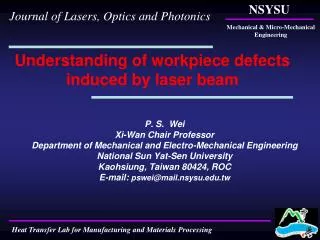
Conceptual Model of Factors that Affect the Mix of Health Human Resources and Quality of Collaboration in Interdisciplinary Primary Mental Health Care Delivery(from Mulvale & Bourgeault 2007)
CIHR/Health Canada HHR Chair Program • I will specifically target the Chair towards investigations of: • HHR competencies, curricula, entry-to-practice requirements for • New providers and new roles for existing providers; • Collaborative practice & innovative models of care; and • Health professionals educated outside of Canada • The contextual factors influencing the deployment of these new recruitment and retention initiatives, locally, regionally, nationally and globally; and • The assessment of ongoing mechanisms to identify, track, acquire, transfer and exchange this new HHR knowledge in a more coordinated fashion.
Previous/Ongoing Research • new providers and new roles for existing providers • History of the Nurse Practitioner Initiative in Ontario (1993-1996) SSHRC SRG (Supervisor) • The Integration of Midwifery in Ontario and British Columbia (1997-2000) SSHRC SRG • Clinical Nurse Specialists and Nurse Practitioners Roles in Canada: a National Systematic Review (2008-10) ONP & CHSRF
Previous/Continuing Research • collaborative practice models of care • Deciding Who Does What, Where and Why? The Influence of Gender and Geographic Location on Efforts to Rationalize the Health Care Division of Labour in Canada & the U.S. (2000-5) • Primary care – with a focus on PHCNPs and PAs • Maternity care – with a focus on midwives/nurse-midwives • Mental health care – with a focus on psychologists
Previous/Continuing Research • The Role of Migrant Care Workers in Ageing Societies: The Canadian Context(2007-8) SSHRC-IOF • This study adds a Canadian component to an international comparative study examining the following issues in the U.K., Ireland and the U.S: • The factors determining the demand for foreign workers in the health care of older people; • The impact of foreign workers on the structure of care and independent living of older people; • The impact of foreign care workers on older people and their families and quality of care • The migration and work experiences of foreign care workers: the means and motivation for migration, role of recruitment agencies, choice of employment and working life
Previous/Continuing Research • Brain Drain, Brain Gain or Brain Waste: A Comparative Examination of Health Care Providers Who Migrate To Canada(2006-9) SSHRC-SRG • In this study, we examine: • the policy, the decision-making processes and regulatory environments addressing the issue of the immigration of physicians, nurses and midwives into Canada; • the experiences of immigrant physicians, nurses and midwives who are included and excluded from practicing in Canada; and ; • the factors influencing immigrant health care providers relative successful at becoming integrated into the Canadian health care system.
Reports from previous two studies Video clips from YouTube on HWM Bibliography on HWM Key links www.healthworkermigration.com
Ongoing Research • On the Move: The Migration of Health Care Providers into and out of Canada, the U.S., the U.K., and Australia(2006-10) CIHR • this study aims to critically examine from a comparative perspective: • the various stakeholders involved in the migration of physicians and nurses into and out of Canada, the U.S., the U.K., and Australia; • the perspectives, positions, interrelations and influences of these various stakeholder groups on the framing of policy ‘problems’ pertaining to health care provider migration and on the overall policy process; • the regulatory environments and broader policy contexts in Canada, the U.S., U.K. and Australia; and finally, • the resultant policies in each of these four countries.
Ministry of Health and Long Term Care Research networks
Applied Health Research Networks Initiative (AHRNI) Structure Population Health Interventions Primary Health Care System Transitions of Prevention & Care Applied Health Research Network Hubs Patterns & Pathways of Inequities SIIReN System Innovation and Integration Research Network PHIRN Population Health Improvement Research Network Systems of Prevention & Care Aboriginal Health Research Team Performance Measurement/ Innovation Team Community Partners Ministry of Health & Long-Term Care Local Health Integration Networks Francophone Health Research Team (RRASFO) Health Human Resources Research Team (OHHRRN) Multicultural Health Research Team (OMHARN)
Goals of OHHRRN • To undertaking more and better health human resource research in Ontario/with an Ontario focus • Leverage funds from OHHRRN vis-a-vis other sources • To enhance capacity in health human resource research in the province • Research production capacity building • Community receptor capacity enhancement • To inform policy and practice regarding health human resources
Balance of Ministry Responsive & Investigator Driven Research • Each network is to devote approximately 60% of its activities towards Ministry Responsive Research (MRR) and 40% towards Investigator Driven Research (IDR) • The kind of KTE Tools discussed by the Ministry can be categorised primarily in terms of time: • Rapid Response – • Technical Briefing – • Knowledge Synthesis – • All members of the networks could be contacted to undertake these – brokered through the network hubs
Principle Successes Database of researchers Knowledge translation tools Research Partnerships
OHHRRN Online Database Directory • OHHRRN Members • Total Number of Members: 105 • Number of Scientists: 53 • Number of Affiliates: 52
Knowledge Translation/Dissemination Tools/Resources: Database Directory Partners Database (Public) Members Database (Private) information is only shared with other members of OHHRRN (i.e. not available on the public database) enables researchers to view/access member information from both partner and member databases Members Database Members: 51 • information is publically shared on the OHHRRN website (i.e. anyone visiting the website can view this information). • enables researchers to view/access information from the partners database only. • Partners Database Members: 54
KnowledgeTranslation/Dissemination Tools/Resources: Website • OHHRRN’s Website • Database Directory: Key HHR Researchers, Experts, Decision Makers • Up-to-date HHR Information: Articles/Publications /Events/ • HHR Opportunities: employment/ research/funding • Links: other relevant HHR websites • HHR Data Directory: Clearing house of HHR Data www.rorrhs-ohhrrn.ca
KT & Dissem.Tools/Resources: OHHRRN Quarterly Newsletter • Recent Updates/Developments at OHHRRN: • Progress updates: OHHRRN’s successful proposal applicants, membership drive, KT tools, • OHHRRN Research: Latest MRR and investigator driven research • Showcasing Ontario’s Latest HHR Research • HHR related research, tools, events, • Upcoming Fireside Chats: HHR related topics • Upcoming Events/Presentations • Spotlighting Ontario’s HHR Experts and New Talent
OHHRRN-MOHLTC: RHPA Large Scoping Review Large Scoping Review: Evaluating the effects of legislative and program changes on health profession regulation in Ontario. • How can we measure the impact of legislative and program changes on: a) the culture of the health education and care systems, and b) the way healthcare is delivered? • What data are available and able to be efficiently and cost-effectively collected and maintained, and what indicators might be used to identify cultural / behaviourial change? • How can we determine whether observed shifts in system culture / behaviour are related to the legislative and program changes? How can we control for environmental impacts on change that were not a result of the legislative and program changes? • Can we obtain early results to help adjust and guide future efforts to achieve the policy objectives?
OHHRRN-MOHLTC: RHPA Large Scoping Review • The Scientific Director of OHHRRN and the Ontario Research Chair in Health Human Resources (ORC-HHR) • Design overall framework to the evaluation of legislative changes pertaining to bills 171 and 179 through selected case studies including: a) regulatory changes to existing regulated health professions of optometry, pharmacy and physiotherapy; b) newly regulated health professions including kinesiology and pharmacy technicians; and c) regulatory changes requiring Colleges to address the barriers to interprofessional practice initiatives. • Discussions continue with the MOHLTC to confirm the details and extent to which the scoping review will take place.
Data Accessibility and Quality • Drawing upon existing data sets through regulatory and licensing bodies • Partnering with other organizations like CIHI and ICES • Working on a HHR Data Directory • Measurement issues • FTEs by profession • How to ‘measure’ productivity
Challenges in HHR Domain • There are critical HHR issues which has led to an increase in research, but often of an uncoordinated nature. • Efforts are underway to begin to better coordinate these efforts at the national level; • A collaborative provincial network would be better positioned to create linkages to other networks nationally and internationally; these efforts would also better enable Ministry responsiveness. • There is a general lack of capacity in HHR research both within the academic/research and policy/decision-maker communities • There are a variety of neglected content areas which a coordinated network would be better able to address.
Health Canada Contribution Agreement CIHR Network Catalyst Grant Developing a Pan-Canadian Health Human Resource Research Network (CHHRRN)_________________________________________________________________
The context of HHR issues in Canada The objectives & approach of CHHRN Outline
Why an HHR Network? • Most major health care system policy issues implicate, or are entirely about HHR. • This is largely because the bulk of health sector expenditures involve the direct costs for HHR including salaries, wages, fees and contracts, and the indirect costs for the training, planning, regulation and management of the health work force as well as workplace environment issues. • Despite the sizeable and growing amount of resources devoted to HHR, Canada nevertheless seems to fluctuate between periods of shortage and surplus. • Faced with continuous and critical HHR issues, jurisdictions across Canada are in need of ready access to the latest information about innovative HHR policies and practices.
The Key Challenges: • There are three main challenges: • 1) there are too few researchers dedicated exclusively to the study of critical HHR issues; • 2) there are a multitude of professional, regulatory and educational stakeholders involved in decisions regarding HHR issues often working in isolation; and • 3) there are too few pan-Canadian opportunities for sharing, learning, and collaborating amongst HHR knowledge users and researchers.
The Key Consequences: • Moveover, • there are few mechanisms for taking innovations developed and lessons learned in one jurisdiction and scaling them up to a pan Canadian level, and there is no formal mechanism for examining common cross-jurisdictional issues. • As a result of these challenges, • there are many instances of a duplication of effort; promising practices far too often go unnoticed; and scarce health human resources are not utilized as efficiently as they otherwise could.
The Canadian HHR Context • The key strategic directions identified in report after report are toward a more effective and collaborative pan-Canadian HHR policy, planning and management to ensure an adequate supply and appropriate mix and distribution of health care professionals working together to address population health needs (e.g.,Bloor & Maynard, 2003; CHSRF 2003; CIHI, 2007; HCC 2005a, 2005b; O’Brien-Pallas, 2007). • Indeed, every “Listening for Direction” exercise undertaken since its inception has HHR issues as the top priority areas as identified primarily by policy- and decision-makers (CHSRF 2001, 2004, 2008).
The Global HHR Context • The WHO has identified HHR as a critical issue, dedicating its 2006 World Health Report to this topic launching the Health Workforce Decade (2006-2015). • The report outlines a 10-year action plan calling for national leadership to initiate and maintain country-based initiatives addressing health workforce needs for increased implementation of effective workforce strategies; increased investments in the workforce; elimination of waste; and strengthening of educational institutions. • This commitment was most recently reiterated in the adoption of the WHO Code of Practice on the Ethical Recruitment of International Health Personnel in May 2010. • Some of the key principles in this document include a call for jurisdictions to become more self-sufficient in HHR; to enhance the collection and analysis of data on HHR; and that HHR changes should be evidence-based and subject to ongoing monitoring.
Recent Developments in the Canadian HHR Context • In 2002, the Advisory Committee on Health Delivery and Human Resources (ACHDHR) was established by the Conference of Deputy Ministers of Health. The ACHDHR reported that a more collaborative, pan-Canadian approach would have immediate benefits • At their meeting in September 2004, the First Ministers agreed to: "continue and accelerate their work on health human resources action plans and initiatives to ensure an adequate supply and appropriate mix of health care professionals"; and "foster closer collaboration among health, post-secondary education and labour market sectors”.
Recent Developments in the Canadian HHR Context • In 2005, a Framework for Collaborative Pan-Canadian Health Human Resources Planning was published (and revised in 2007). • This framework includes a set of specific goals and objectives that span the short, medium and long term that move us away from more utilization-based planning undertaken in isolation with a lack of awareness for of the impact on the system of health professions. • The benefits of a systems-based, collaborative approach are many but it relies on the combined efforts of numerous professional and regulatory stakeholders, provincial/territorial ministries of health, and other key actors within the health care system (educational institutions, local governments and private sector organizations). • Critical success factors include appropriate stakeholder engagement, strong leadership, a clear understanding of roles/responsibilities, and a focus on cross-jurisdictional issues.
Recent Research Developments in the Canadian HHR Context • Concurrently, several HHR syntheses have been undertaken from 2003, commissioned by a range of stakeholders, including: • CHSRF, CPRN, HCC, Health Canada, MSFHR addressing a range of topics including: • healthy work environments • HHR modelling/forecasting • HHR productivity • team-based care & innovative staffing models
Recent Developments in the Canadian HHR Context Over this same time frame, regional networks have been developed: • The Ontario Health Human Resources Network (OHHRRN) is a province-wide network linking HHR researchers and community decision-makers and partners with the goal of creating and synthesizing high-quality research that addresses complex issues that affect HHR planning and management. • The Western and Northern Health Human Resources Planning Forum (WNHHRPF) provides information exchange, networking, communication and supports a wide range of collaborative multi-jurisdictional HHR projects. • The Atlantic Advisory Committee on Health Human Resources (AACHHR) is comprised of representatives from the four Atlantic Provinces, and serves as a resource and source of policy advice to Atlantic deputy ministers of health and of education to enhance cooperation on issues relating to HHR planning.
Recent Developments in the Canadian HHR Context • “PROMOTING INNOVATIVE SOLUTIONS TO HEALTH HUMAN RESOURCES CHALLENGES”2010, HoC Standing Committee on Health Report • “It is clear from the Committee’s study that thinking boldly and broadly about HHR is necessary to develop local and unique solutions that involve a wide range of health professionals from midwives to health information managers. The Committee learned that these innovative solutions have been made possible by continued collaboration and financial investments made by the federal government and the provincial and territorial governments, which began with the 2003 and 2004 agreements on health care reform. However, it remains clear that sustained results in addressing HHR challenges in Canada requires on-going collaboration between different levels of government, as well as leadership from the federal government in providing sustained and secure funding mechanisms ... The federal government needs to be more effective in its promotion of collaborative planning in HHR with interested jurisdictions, either through existing mechanisms or the establishment of new ones.”
Our Objectives: • The main objective of the pan-Canadian HHR Network is to create the virtual infrastructure to better share HHR knowledge, innovation and promising practices by: • first, creating a dynamic network of regionally- and thematically-based HHR researchers and knowledge users and clinical, policy and program decision-makers across Canada so as to better coordinate and capitalize upon their complementary areas of expertise and knowledge needs; • second, linking up these networks of HHR researchers and key knowledge users and decision-makers through a state of the art, interactive web-based portal to better share knowledge and lessons learned and identify strategic areas for knowledge synthesis and future applied HHR research; and (i.e., electronic communities of practice) • third, creating a ‘clearinghouse’ of Canadian and international HHR research, knowledge and promising practices available in a variety of user-friendly formats.
Contact us: OHHRRN: info@rorrhs-ohhrrn.ca CHHRN: info@hhr-rhs.ca Thank You!!!