Download
1 / 29
290 likes | 296 Views
Auto-antibodies in HIV: Rheum for confusion. Riëtte du Toit Division of Rheumatology Tygerberg Hospital. Rheumatology in the HIV pandemic. Unique to HIV HIV ass arthritis Painful articular sy DILS. Associated with HIV Spondyloarthropathies Vasculitis Myopathy / myositis etc

E N D
Auto-antibodies in HIV:Rheum for confusion Riëtte du Toit Division of Rheumatology Tygerberg Hospital
Rheumatology in the HIV pandemic Unique to HIV HIV ass arthritis Painful articular sy DILS Associated with HIV Spondyloarthropathies Vasculitis Myopathy / myositis etc Fibromyalgia IRIS Rheum arthritis SLE Sjogrens Sarcoid Immuno-suppression Treatment related Myopathy Gout AVN Rheuma syndromes – 10% (up to 60%) of patients
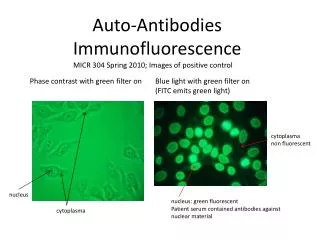
Presence of auto-antibodies in HIV Massabki et al. AIDS 1997;11:845-1850
Mechanism of auto-antibodies • Cross reaction between virus and self-Ag • Polyclonal hyperglobulinemia • In 45% of patients • Associated increased levels of immune complexes • Immune dysregulation, loss of tolerance Zandmann-Goddard G et al. 2002. Autoimm Rev: 329-37
Which ? ANA, a-DsDNA, a-Sm, a-U1 RNP, a-Ro / a-La ANCA ACA, LA RF, aCCP Cryoglobulins Massabki et al. AIDS 1997;11:845-1850 Du Toit et al. J Rheumatol 2011;38:1055-60
Significance? Usually low titre occurring in advanced disease / low CD4 May disappear with immune reconstitution Does not correlate with immunoglobulin levels Has been ass with increased mortality Massabki et al. AIDS 1997;11:845-1850 Du Toit et al. J Rheumatol 2011;38:1055-60
Clinical correlation Spondyloarthropathies Inflammatory polyarthritis Systemic lupus erythematosus DILS v Sjogrens Antiphospholipid antibodies and thrombosis Vasculitis and ANCA
Auto-antibody interpretation 1. Spondyloarthropathies • Prev rare in Africa; emerged with HIV • Often undiff; Also ReA / PsA • Occurs in advanced HIV infection • HLA-B27 – antigen / allele • Frequency +: 70-90% • Dependant on ethnicity • Pts of African descend often not HLA-B27+ • HLA-B5703 ass with SpA in Africa, protective against HIV Lothrenoo et al. Curr Op Rheum 2008;20:92-99 Reveille et al. Sem Arthr Rheum 2000;147-66 Savige et al. Autoimmunity 1994;18
2. Inflammatory polyarthritis: RA and related auto-antibodies • RA tend to remit in advanced HIV disease • De novo / flare with IRIS / HIV elite controller • In advanced HIV: • Polyarthralgia common (45%) • HIV associated arthritis • varies from oligo to polyarthritis • Usually self limiting • Other: associated with viral infections, gout • RA-serology in HIV: • RF • ACPA Iordache L et al. Autoimm Rev 2014; 13:850-57.
Case 1 • 37 yr old male • HIV +, not on ARV’s • CD4: 320 • 3 month history • Painfully swollen wrist, MCP’s • Significant functional loss • No extra-articular / systemic features • ESR 60mm/h • RF: 20.7 IU/ml • aCCP: >250 IU ? RA presenting atypical in HIV patient?
Rheumatoid factor in the setting of HIV • RF = Ab against Fc-portion of IgG • RF (IgM) + in 47% of patients with HIV • Low titres
ACPA • False + in: • Psoriatic arthritis 8% • SLE 3% • 1° Sjogrens 8% • Pulmonary TB 32% Annals of Internal Medicine: Meta Analysis 2007 Clin Rheum 2008 Ann rheum dis 2006 J Rheum 2011 Antibody against citrullinated peptides (fillagrin, vimentin) Specifity for RA: up to 99% (general population) Predictive of future RA
RA and related auto-antibodies • Both RF (47%) and aCCP (15%) false + in advanced HIV • Titres negatively correlate with CD4 when on HAART • Not associated with clinical RA • Doesn’t predict the development of RA during immune reconstitution • Pulmonary TB: • aCCP 32% + • RF 62% + Kakumanu et al. Arthritis Rheum 2008;58:1576-81
3. Lupus v HIV SLE is a CD4 driven disease…remits in advanced HIV Two great mimickers Fever, weight loss, lymphadenopathy Alopecia; Photosensitivity; vasculitic rash Thrombosis Arthritis; myositis Nephropathy Lymphopenia; ITP; AIHA;
Case 2 • 26 Yr old female • Known SLE (5 years) • photosensitivity, alopecia; arthritis • Lymphopenia • ANA (320); aDs DNA+ • Treatment: • Chloroquine • Prednisone 7.5mg • Presented with • Weight loss, fever • Gen lymphadenopathy
Laboratory Lymphopenic ANA, aDs DNA + C3, C4 low HIV + (ELISA) Lupus v HIV v both?
HIV+ patient: ANA • ANA + in up to 17-23% (advanced HIV) • A-Sm and a-DsDNA may also be + • Usually low titres • Remember: SLE tends to remit in advanced HIV • Low complement rarely occurs in HIV SLE: HIV Ab • ELISA: • may be false positive • 4th Gen combination assay • False pos / indeterminate • Western Blot (Ab against p24, p31, gp41, gp120/160): • Reports of cross reactivity (p24, gp41) • Confirmation: • PCR , Viral load Esteva HM et al. Ann Rheum Dis 1992;51:1071-73
4. DILS v Sjὂgrens in the HIV + patient(diffuse infiltrative lymphocytosis syndrome) Prevalence 4-8% Revelle JD et al. Semin Arthr Rheum 2000;30:147-166 Smith PR et al. J Clin Path 2000;53:177-181
5. Antiphospholipid antibodies (AP Ab) and thrombosis in HIV • Thrombosis – up to 7% of HIV advanced patients • Theories: decreased anticoagulant activities due to deficiencies in protein S, protein C, anti-thrombin, • Endothelial damage – HIV itself • Thrombosis correlates with CD4, opportunistic infections and malignancy • AP Ab in general population • AP Ab often transiently positive after an infection • IgM less specific than IgG Zandman-Goddard et al. Autoimmunity Reviews 2002;1:329-37 Reveille et al. SemArthr Rheum 2000;147-66 MW Saif. Aids patient care 2001;6:311
Antiphospholipid antibodies in HIV: • ACA • IgM and IgG in up to 65 - 95% of patients • usually not B2-GP1 dependant • LA • in +- 45% of patients • Had been associated with PJP infection • anti-B2 GP1 • In 5 - 65% • Advanced HIV • Likely triggered by infection • NOT associated with thrombosis Zandman-Goddard et al. Autoimmunity Reviews 2002;1:329-37 Reveille et al. Sem Arthr Rheum 2000;147-66
6. Vasculitis in HIV • Most vasculitides had been described in HIV • Prevalence of 1-23% • May occur at higher CD4 counts • Often fulfils criteria for a distinct category Giant cell arteritis Takayasu’s arteritis PolyarteritisnodosaBehcet’s syndrome Kawasaki’s disease Hypersensitivity vasculitis Henoch-Schὂnlein purpura Granulomatosis with Polyangiitis Isolated CNS angitis Reveille et al. Sem Arthr Rheum 2000;147-66
ETIO: • HIV itself; immune complex mediated • Other co-infections HBV / HCV • Drug reaction • Mimics: TTP, DIC • Treatment : ARV’s , often combined immunosuppressants
ANCA associated vasculitis • + c-ANCA and p-ANCA in HIV patients • Indirect immunofluorescence • + in 20-30% of Symptomatic HIV infected patients • Atypical pattern - 60% • Peri-nuclear - 30% • Cytoplasmic - 10% • Target Ag (ELISA) • Identified in 33% of cases (often atypical) • Savige et al: • a-MPO + in 25% • Absence of clinical vasculitis Palpable purpera + ANCA = vasculitis Cornely OA et al. 1999. Infection;27:92-96. Klaassen RJL et al. 1992 ClinExp Immunol;87:24-30 Savige JA et al. Advances in Experimental Medicine and Biology. DOI 10.1007/978-1-4757-9182-2_58
In conclusion In advanced HIV • Variety of rheumatological manifestations • RA, SLE remits, • others occur with increased frequency / associated with advanced disease • Auto antibodies are common • Usually low titres, IgM • Often transient • as CD4 increases (HAART) • Related to other infections • Typically not associated with clinical disease
In practice… • Take care not to use Ab’s as “random screening” • Take CD4 into consideration • Consider concomitant infections • HBV, HCV, TB! • Look for alternative evidence • Histology , cultures • Complement
In patients presenting with features of a connective tissue disease • Exclude HIV as a mimicker of CTD • and visa versa • May co-exist HAART may resolve the “CTD” where as inappropriate immunosuppression may be fatal for the HIV-infected patient