Download
1 / 18
180 likes | 182 Views
This presentation by William Jagust discusses the potential of PET as a surrogate marker in Alzheimer's disease (AD), highlighting its ability to assess tissue biochemistry and predict cognitive decline. It also explores the relevance of PET tracers and their correlation with AD pathology. However, the presentation acknowledges the need for further validation and standardization in order to fully incorporate PET in clinical trials for AD.

E N D
Presented by William Jagust, M.D. at the November 18, 2002 Peripheral and Central Nervous System Advisory Committee meeting
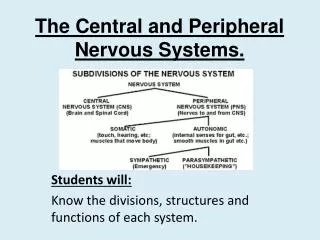
Why is PET a Good Potential Surrogate Marker in AD? • PET is a good assay for tissue biochemistry and physiology that is related to disease process • PET is highly related to cognitive function and predictive of cognitive decline • PET is sensitive, reliable, and valid as a marker for AD pathology • PET provides statistically powerful measures of decline
PET Tracers Relevant to AD • Radioligands that bind to acetylcholinesterase • Reflect cholinergic function • Radioligands that bind to amyloid • Reflect unknown characteristics of amyloid pathology • Fluorodeoxyglucose • Synaptic activity
Cholinergic Ligands in AD Kuhl et al, Neurology 1999
Markers of Alzheimer’s Disease: Temporal-Parietal Hypometabolism C AD1 AD2
FDG PET and AD Diagnosis • Hoffman et al., J Nucl Med 2000 (N=22) • Pathologically confirmed AD • sensitivity 90%, specificity 65% • Silverman et al., JAMA 2001 • Progressive dementia (N=146) • sensitivity 93%, specificity 76% • Pathologically confirmed AD (N=138) • sensitivity 94%, specificity 73%
FDG-PET Predicts Decline • Baseline PET predicts MMSE change in AD patients (Jagust et al., 1996) • Baseline PET predicts decline from memory-impairment to dementia (Minoshima et al, 1997) • Baseline PET predicts memory decline in nondemented ApoE4 carriers (Small et al, 2000) • Baseline PET predicts decline from normal to MCI (DeLeon et al., 2001)
PET Metabolic Rates Predict Rate of Decline in AD MMSE Change r=0.58 Post Temp Ctx rCMRglc (mg/100g/min)
0.8 0.8 0.7 0.7 0.6 0.6 0.5 0.5 0.4 0.4 0.3 0.3 0.2 0.2 .55 .60 .65 .70 .75 .80 .85 .90 .95 .7 .8 .9 1.0 1.1 1.2 1.3 Regional Glucose Metabolism is Correlated with Cognitive Function Delayed Recall Delayed Recall left temporal lobe left hippocampus
2-year Glucose Metabolic Decline in Asymptomatic ApoE 4 Heterozygotes P < 0.001 Reiman et al., PNAS 2001
Asymptomatic Subjects Per Treatment Group to Detect a Drug Effect in Two YearsPost Cingulate rCMRglc, 80% Power, p = 0.01, two tailed Number of Subjects Reiman et al, PNAS 2001 Estimated Drug Treatment Effect
AD Patients per Treatment Group to Detect a Drug Effect in 1 yearFrontal rCMRglc, 80% Power, p = 0.01, two tailed Number of Subjects Estimated Drug Treatment Effect Reiman et al
FDG-PET as a Surrogate: PositivesLink between PET and clinical decline • PET predicts clinical decline • Biologically plausible – “on the pathway for AD” • sensitive and specific for pathology • related to pathology, synaptic function • correlated with cognition • Statistically powerful
FDG-PET as a Surrogate: NegativesLink Between PET and Disease Modification • Problem • Inability to distinguish symptomatic from disease-modifying drug effects • Solutions • Randomized start or withdrawal design • Use PET tracers that reflect basic biology of AD: amyloid imaging agents • Assess PET in symptomatic drug treatments
Technical Considerations • Standardization of multisite acquisition • state • input function • attenuation correction • resolution • Standardization of data analysis • quantitation: metabolic rates, ratios • regions-of-interest, atlas and voxel-based
Summary • FDG PET shows potential as a surrogate but clearly has not been confirmed • Very sensitive in detecting decline, and statistically powerful • Strong links with clinical symptoms and pathology, questions on disease modification • Incorporation of PET in clinical trials will help address questions