Download
1 / 1
20 likes | 131 Views
Confirmatory Factor Analysis of the SCARED in a Pediatric Chronic Pain Sample: Implications for Use. Jevans@Alliant.edu. PAN. .93 (.96).

E N D
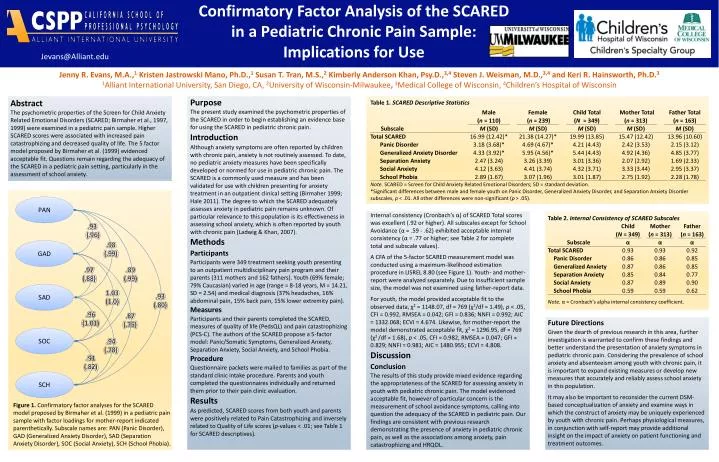
Confirmatory Factor Analysis of the SCARED in a Pediatric Chronic Pain Sample: Implications for Use Jevans@Alliant.edu PAN .93 (.96) Jenny R. Evans, M.A.,1 Kristen Jastrowski Mano, Ph.D.,1 Susan T. Tran, M.S.,2Kimberly Anderson Khan, Psy.D.,3,4 Steven J. Weisman, M.D.,3,4 and Keri R. Hainsworth, Ph.D.3 1Alliant International University, San Diego, CA, 2University of Wisconsin-Milwaukee, 3Medical College of Wisconsin, 4Children’s Hospital of Wisconsin .98 (.99) GAD .97 (.88) .89 (.99) SAD Purpose The present study examined the psychometric properties of the SCARED in order to begin establishing an evidence base for using the SCARED in pediatric chronic pain. Introduction Although anxiety symptoms are often reported by children with chronic pain, anxiety is not routinely assessed. To date, no pediatric anxiety measures have been specifically developed or normed for use in pediatric chronic pain. The SCARED is a commonly used measure and has been validated for use with children presenting for anxiety treatment in an outpatient clinical setting (Birmaher 1999; Hale 2011). The degree to which the SCARED adequately assesses anxiety in pediatric pain remains unknown. Of particular relevance to this population is its effectiveness in assessing school anxiety, which is often reported by youth with chronic pain (Ladwig & Khan, 2007). Methods Participants Participants were 349 treatment seeking youth presenting to an outpatient multidisciplinary pain program and their parents (311 mothers and 162 fathers). Youth (69% female; 79% Caucasian) varied in age (range = 8-18 years, M = 14.21, SD = 2.54) and medical diagnosis (37% headaches, 16% abdominal pain, 15% back pain, 15% lower extremity pain). Measures Participants and their parents completed the SCARED, measures of quality of life (PedsQL) and pain catastrophizing (PCS-C). The authors of the SCARED propose a 5-factor model: Panic/Somatic Symptoms, Generalized Anxiety, Separation Anxiety, Social Anxiety, and School Phobia. Procedure Questionnaire packets were mailed to families as part of the standard clinic intake procedure. Parents and youth completed the questionnaires individually and returned them prior to their pain clinic evaluation. Results As predicted, SCARED scores from both youth and parents were positively related to Pain Catastrophizing and inversely related to Quality of Life scores (p-values < .01; see Table 1 for SCARED descriptives). 1.03 (1.0) Abstract The psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED; Birmaher et al., 1997, 1999) were examined in a pediatric pain sample. Higher SCARED scores were associated with increased pain catastrophizing and decreased quality of life. The 5 factor model proposed by Birmaher et al. (1999) evidenced acceptable fit. Questions remain regarding the adequacy of the SCARED in a pediatric pain setting, particularly in the assessment of school anxiety. .93 (.80) .96 (1.01) .87 (.75) SOC .94 (.78) .91 (.82) SCH Internal consistency (Cronbach’s α) of SCARED Total scores was excellent (.92 or higher). All subscales except for School Avoidance (α = .59 - .62) exhibited acceptable internal consistency (α = .77 or higher; see Table 2 for complete total and subscale values). A CFA of the 5-factor SCARED measurement model was conducted using a maximum-likelihood estimation procedure in LISREL 8.80 (see Figure 1). Youth- and mother-report were analyzed separately. Due to insufficient sample size, the model was not examined using father-report data. For youth, the model provided acceptable fit to the observed data, χ2 = 1148.07, df = 769 (χ2/df = 1.49), p < .05, CFI = 0.992, RMSEA = 0.042; GFI = 0.836; NNFI = 0.992; AIC = 1332.068; ECVI = 4.674. Likewise, for mother-report the model demonstrated acceptable fit, χ2 = 1296.95, df = 769 (χ2 /df = 1.68), p < .05, CFI = 0.982, RMSEA = 0.047; GFI = 0.829; NNFI = 0.981; AIC = 1480.955; ECVI = 4.808. Discussion Conclusion The results of this study provide mixed evidence regarding the appropriateness of the SCARED for assessing anxiety in youth with pediatric chronic pain. The model evidenced acceptable fit, however of particular concern is the measurement of school avoidance symptoms, calling into question the adequacy of the SCARED in pediatric pain. Our findings are consistent with previous research demonstrating the presence of anxiety in pediatric chronic pain, as well as the associations among anxiety, pain catastrophizing and HRQOL. Future Directions Given the dearth of previous research in this area, further investigation is warranted to confirm these findings and better understand the presentation of anxiety symptoms in pediatric chronic pain. Considering the prevalence of school anxiety and absenteeism among youth with chronic pain, it is important to expand existing measures or develop new measures that accurately and reliably assess school anxiety in this population. It may also be important to reconsider the current DSM-based conceptualization of anxiety and examine ways in which the construct of anxiety may be uniquely experienced by youth with chronic pain. Perhaps physiological measures, in conjunction with self-report may provide additional insight on the impact of anxiety on patient functioning and treatment outcomes. Figure 1. Confirmatory factor analyses for the SCARED model proposed by Birmaher et al. (1999) in a pediatric pain sample with factor loadings for mother-report indicated parenthetically. Subscale names are: PAN (Panic Disorder), GAD (Generalized Anxiety Disorder), SAD (Separation Anxiety Disorder), SOC (Social Anxiety), SCH (School Phobia).



















