Download

1 / 14
140 likes | 198 Views
R. Rodriguez-Garcia 1 , O. Kayode 2 ,

E N D
R. Rodriguez-Garcia1, O. Kayode2, B. Manteuffel3, A. Seymour4, B. Simms5, B. de Zalduondo6, R. Bonnel1, N. Njie1 1The World Bank, Washington, United States, 2NACA, Abuja, Nigeria, 3IFC Macro, Atlanta, United States, 4DFID and 5UK Consortium on AIDS and International Development, London, United Kingdom, 6UNAIDS, Department of Evidence, Geneva, Switzerland • July 26, 2012 Evidence for Community Participation in Policy Dialogue from the Evaluation of Community Responses to HIV and AIDS
Rationale of the Evaluation Is the community response delivering results and Value for Money? • How much money is available for the community response? How much at the community level? • What are the results of these investments? • Knowledge about HIV and AIDS • Behavior • Access to and utilization of HIV/AIDS/health services • Outcomes: Social change and health related We did NOT evaluate donors programs
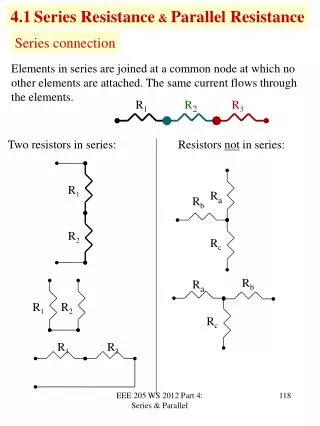
Community responses range from informal to formal Government
Community responses can mobilize substantial resources • In 2003-2009 international funding amounted to at least US$600 million per year for the civil society response • These funds reach mainly international and large NGOs at national level • CBOs annual budgets: US$10,000 (Kenya) to US$16,000 (Nigeria) • Small NGOs and CBOs mobilize international and domestic resources
The Community Rely on Volunteers to Provide Services (Kenya 2010) Estimated value of unpaid volunteers as % of CBOs and NGOs financial resources Annual Budgets: (< $6,000) ($72,000) ( $660,000) • CBOs increase their total resources by mobilizing volunteers –caregivers-community based workers-- which represents a 30% to > 100% in CBOs’ resources in Kenya, Nigeria and Zimbabwe
Allocation of resources by CBOs(Kenya, Nigeria, Zimbabwe) Most funding is allocated to: • Management and capacity building (29%) • Impact mitigation (27%) • Prevention (24%) • Treatment and care (20%) • Is this allocation generating corresponding results? Source: Survey of NGO/CBOs in Kenya, Nigeria and Zimbabwe (2011) by the World Bank with IFC Macro.
Efficiencies can be Improved by Shifting Focus to a Combination of Activities aligned to the Epidemic Percentage of CBOs Engaging in Specific Activity Categories, Adamawa, Nigeria. Percentage of Total CBO Expenditures by Categories, Adamawa, Nigeria.
Community Response to HIV and AIDS - Evaluation Findings Show: 1 • Strong casual evidence that specific community interventions can affect the course of the HIV epidemic through: • Increased HIV knowledge- Kenya, Burkina increased condom use - Kenya, India, Zimbabwe increased HCT uptake -Senegal, Zimbabwe, and increased access and use of services -Nigeria, Zimbabwe, South Africa • It can also increase PMTCT and improve HIV/AIDS and health outcomes by contributing to reducing HIV incidence (Zimbabwe, 1990,-200s), and lowering STIs prevalence (India)
Community Response to HIV and AIDS - Evaluation Findings Show: 2 • Strong relationship evidence that community-based actions play a pivotal complementary role to national programs by providing services to communities which otherwise would have been left without access to services such as: • rural communities - Nigeria • high risk groups - India, Zimbabwe • However, there is mixed evidence on social change outcomes – Stigma, domestic abuse, gender. • Gender matters. Women in community groups adopted low-risk behaviors faster lower HIV incidence in the early 2000s – Zimbabwe.
Evaluation Methodology supportsconfidence on findings • Multi-country: Eight countries • Burkina Faso, India, Kenya, Lesotho, Nigeria, Senegal, South Africa, Zimbabwe • Mixed-method: Seventeen studies • Country evaluations (mix of RCT, quasi-experimental, cross-sectional and longitudinal ) • Analysis of funding flows and CBOs budgets • Qualitativeanalysis • Cross-cutting studies - triangulation • Multi disciplinary research teams • Consultative Process – national specialists &CSOs
Key Conclusion: CR better when responding to a crisis or introducing a new service • What is the fundamental goal of community-based activities? To improve implementation? To facilitate integration? • To complement and provide more services? – services expansion • To provide similar services to more people in more areas? – services extension • To provide services that the health system is not providing (more groups or geographical areas)? – filling health services gaps • Strengthen the community itself? – mobilization for advocacy • How to increase Community responses efficiencies? • With TA that is focused, related to specific objectives, and with realistic expectations as to results. • Align community-based support to the epidemic • Balance efficiency and effectiveness with equity • Plans for regular evaluations of results should be more systematic, not more complex
Implications for community programming – Use the Evidence! • Examine: (i)role and compensation of volunteers and (ii) stigma • Focus on (i) realistic goals that community-level workers can achieve and (ii) specific roles in the health sector • Test methods of (i) financing and (ii) capacity strengthening • Provide different types of support for CBOs(i) in communities (defined as groups) and in communities (defined geographically), and (ii) differentiated by gender and cohort (youth)
WEB site: aidsconsortium.org.uk THANK YOU EVALUATION OF COMMUNITY RESPONSES TO HIV AND AIDSFindings TitleSubtitle