Download
1 / 33
340 likes | 625 Views
Male , 36 years of age. Impaired fasting glucose since 1988 (21 years of age) R/ diet alone Lean, 177cm and 57,2 kg, was never obese No complaints, coincidental finding during check up Medical history negative

E N D
Male , 36 years of age • Impaired fasting glucose since 1988 (21 years of age) • R/ diet alone • Lean, 177cm and 57,2 kg, was never obese • No complaints, coincidental finding during check up • Medical history negative • Family history: mother ( age of 50) and sister (after corticosteroids) have diabetes. • 2 healthy children
Lab results • HbA1C 6,6 (4-6) • C-Peptide 2,25 ng/ml (0,8-4,2) • Normal liver function and renal function • No microalbuminuria • Low cholesterol(154 mg/dl), high HDL (50 mg/dl) and low triglycerides • ICA: 12 JDF Units (<12) • GAD65 AB :0,6% (<2,6) • Insulin antibodies 0,5% (<0,6)
Medical therapy • 05/04: Glargine 6 units, Repaglinide 3x2mg /d • 09/04: HbA1C 7,3% • Glargine 8U, lispro with every meal, repaglinide stopped
Maturity-Onset Diabetes of the Young (MODY) • 2-5% of diabetics • autosomal dominant inheritance • onset usually before age 25 • impaired -cell function • normal weight, no islet cell autoantibodies • no insulin resistance
MODY Types • MODY 1: mutations in hepatocyte nuclear transcription factor-4 • (HNF-4) severe -cell secretory defect • MODY 2: mutations in glucokinase mild hyperglycemia • due to -cell reponsiveness to glucose • MODY 3: mutations in hepatocyte nuclear transcription factor-1 • (HNF-1) severe -cell secretory defect • MODY 4: mutations in insulin promoter factor (IPF-1 gene) • MODY 5: mutations in hepatocyte nuclear factor 1 (HNF-1) • severe -cell secretory defect • MODY 6: mutations in neurogenic differentiation factor 1 • (Neuro D1)
Clinical entity of MODY • Early –onset, non insulin-dependent diabetes • Insulin treatment not a requisite 5 years following diagnosis and no significant C-peptide deficit • Autosomal dominant inheritance: at least 2 generations (diagnosis before 25 years) • No acanthosis nigricans, no obesity • No pancreatic auto-antibodies(especially GAD)
Diabetes in Young Adults (15-30 years) Type 2 Type 1 MODY MIDD 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 Age of diagnosis
Diagnosis of diabetes before 25 years in at least 1 & ideally 2 family members Off insulin treatment or measurable C-peptide at least 3 (ideally 5) years after diagnosis Must be diabetes in one parent (2 generations) and ideally a grandparent or child ( 3 generations) Diagnostic criteria for MODY • Early-onset diabetes • Not insulin-dependent diabetes • Autosomal dominant inheritance • Caused by a single gene defect altering beta-cell function, obesity unusual Tattersall (QJM 1974)
The Genetic Causes of MODY MODY 75%Transcription factors 11%MODY x 14%Glucokinase(MODY2) 3%HNF4 3%HNF1 <1%IPF1 <1%NeuroD1 69%HNF1(MODY3) Frayling, et al Diabetes 2001
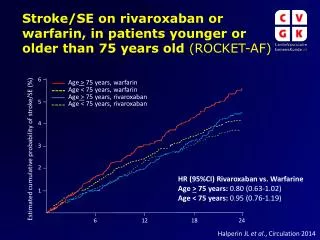
Transcription factor (HNF-1a) Glucokinase Normal Two subtypes of MODY Glucokinase and Transcription factor 20 16 12 Glucose (mmol/l) 8 . . 4 0 0 20 40 60 80 100 Age (yr..) Pearson, et al Diabetes 2001
Glucokinase (MODY 2) • Glucokinase: central role in insuline secretion • Glucose->glucose-6-phosphate->insuline secretion • Expressed in beta cells and hepatocytes • Pancreatic glucose sensor
Glucokinase (MODY2) Rare in hospital diabetic clinicsIncidental hyperglycaemia in childrenCommon in gestational diabetesPersistent raised fasting glucose(99-162 mg/dl) from birth Little rise (54 mg/dl) in OGTT No extra-pancreatic featuresNot obese (usually) Often asymptomatic TEST PARENTS!
Transcription factor MODY • Transcription factors: key role in the regulation of gene expression in development of adult tissue • Reduced maximal insulin secretion • Hepatocyte nuclear factors play a key role in beta-cell development, regulation of proliferation of beta-cells and metabolism in the mature beta cell • Progressive beta cell dysfunction
HNF1a (MODY3) Commonest cause of MODY May be misdiagnosed as type 1 Typically develop 12-30 yr FPG maybe normal initially Large rise (90 mg/dl) in OGTTWorsening glycaemia with age Low renal threshold (glycosuria)Not obese (usually) Parents and grandparents usually diabetic
HNF1α (MODY3) and treatment • Low dose sulfonylureas, first - line medication • Marked sensitivity, should be introduced with caution. • Hypersecretion of insulin, increased sensitivity to the insulin secreted • Metformin not as effective
Differentiating between HNF1a (MODY3) and Glucokinase (MODY 2) based on moderate hyperglycaemia following glucose challenge OGTT ResultsGCK and HNFEuropean MODY Consortium (n =364) - Stride et al Diabetologia 02 Plasma Glucose mmol/l *** HNF1 *** GCK *** p < 0.001
Summary : Glucokinase and Transcription factor diabetes rather than “MODY” MODY Transcription factormutations Glucokinasemutations (HNF-1, HNF-1b, HNF-4) Onset at birthStable hyperglycaemiaDiet treatmentComplications rare Adolescence/young adult onsetProgressive hyperglycaemia1/3 diet, 1/3 OHA, 1/3 InsulinComplications frequent
HNF-1 (MODY 5): Renal Cysts and Diabetes (RCAD) Renal cysts • Often seen on anti-natal scanning - variable • Renal function variable - mild impairment - endstage renal failure 50% require dialysis • Different renal histology Diabetes • Diagnosis 22 (10 - 47) yr., often on insulin Other extra-pancreatic featuresuterine abnormalities, insulin resistance and gout Nishigori et al Diabetes 1998, Lindner et al 1999 Hum Mol Gen Bingham et al 2000 Kidney Int, Bingham et al 2001 AmJ Hum Gen, Bingham et al 2002 Kidney Int,
Young adult diabetes diagnosis : distinction from type 1 and type 2NOT on a single clinical criteriaor a single investigationmulti - facetted approach needed
MODY Type1 Non insulin dependent Yes NoParents affected 1 0-1Age of onset < 25yr Yes YesMODY diagnostic criteria separate well from Type 1
MODY Type 2 Type1 Non insulin dependent Yes Yes NoParents affected 1 1-2 0-1Age of onset < 25yr Yes unusual YesMODY diagnostic criteria do not separate well from early-onset Type 2
MODY Type 2 Type1 Non insulin dependent Yes Yes NoParents affected 1 1-2 0-1Age of onset < 25yr Yes unusual YesObesity +/- + + + +/-Acanthosis -+ + -NigricansRacial groups low high low(Type 2 prevalence)
Clinical Assessment of Non-Type 1Young Adult Diabetes Clinical Assessment - Diabetes characteristics - Non-pancreatic manifestations - Family History Investigations - General & Specific Diagnostic Tests Key for diabetes syndromes
Diabetes + Neurological Obesity ++ Deafness Acanthosis nigricans DIDMOAD MIDD Type A IRLipodystrophy Retinitis pigmentosa OtherCystic fibrosisRenal cysts & Diabetes Prader-Willi AlstromBardet-BiedlLawrence-Moon
MODY Variable Not present Usually detectable(0-1 nmol/l) normal (HDL>1.2 MODY3) Type 1 Variable >95% diagnosis not measurable > 3-5 years (<0.33nmol/l) normal Non genetic Investigations Glycaemia Autoantibodies ICA, IA2 or GAD C peptide Lipids Type 2 Variable unusual detectable may be high (>1nmol/l) HDL low TG high
Criteria distinguishing HNF1a (MODY3) from Type 1 are useless for differentiating from Type 2 young adults! • Familial 2 generations 96% HNF1a 80% Type 2 • 3 generations 74% HNF1a 50 % Type 2 • C peptide present or not insulin 100% HNF1a 100 % Type 2 treated 3 yrs post diagnosis • Pancreatic Auto - antibody -ve 98% HNF1a 90% Type 2 • So use different data for answering different questions!
Distinguishing HNF1a (MODY3) from Type 2 Consider in “type 2” diabetic young adults when…. • Not obese 86% HNF1a 25% Type 2 • Not over weight 64% HNF1a 4 % Type 2 • Not acanthosis nigricans 100% HNF1a 20% Type 2 • HDL > 1.2 mmol/l 83% HNF1a <8% Type 2 • Caucasian 94% HNF1a 30% Type 2 • Consider HNF1a testing in any “Type 2” young adult who is not obese, does not have AN, or low HDL especially if CaucasianUK Data on HNF1a/Type 2 Hattersley, Barrett, Ehtisham, Owen, Pearson unpublished
Genetic Testing: why do it? • Makes diagnosis : defines monogenic and subtype • Differentiates from type 1 • Helps define prognosis • Helps family counselling • Helps treatment decisions: - Glucokinase: safely leave children off treatment - HNF1α: very sensitive to sulfonylureas
MODY: conclusion • Use both diagnostic criteria and clinical information and non-genetic investigation to suggest a diagnosis • Genetic testing makes diagnosis : defines MODY, defines subtype helps with counselling, prognosis and treatment • BUT ….Expensive £1-400- - only do if alter management • Test ordered guided by clinical criteria as to likely gene. Discuss each case before testing