Download
1 / 101
1.01k likes | 1.02k Views
This course explores the concept of clinical governance and its importance in providing patient-centered, accountable, safe, and high-quality healthcare. Topics include service user involvement, use of clinical information, NICE guidance, and more.

E N D
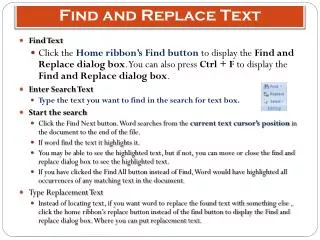
EXAMPLE COURSE EXAMPLE COURSE How to Find Your Way Around… 1. You can play the PowerPoint, and find the Test here 2. You can minimise this column and make the main page bigger by clicking this icon. Click it again to bring it back. 3. Always click this ‘Home’ icon to save your progress and log off. This is very important! EXAMPLE COURSE
If you exit the course before you have completed the PowerPoint you will start from the beginning as the system does not continue from your last point.
Induction - Clinical Programme Part 2 Clinical Governance Medicine Management Supervision NHS Protect Fraud Awareness Occupational Health Complaint Handling Introduction to Learning Disabilities
Clinical Governance What is Clinical Governance? Clinical Governance is about providing a patient-centred, accountable, safe and high quality service in an open and questioning environment. Clinical Governance questions traditional structures and ways of doing things and creates a consistent and sustained approach to improving the quality of healthcare. COURSE OBJECTIVES • What Clinical Governance is; • History of Clinical Governance; • Service User involvement; • PALS involvement; • Use of clinical information; • NICE guidance; • Useful contacts. Definition of Clinical Governance “A framework through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish".
Definition of Quality There have been several definitions of quality care in the last 20 years. The definition below was adopted by the NHS in 2008. Quality treatment and care has three elements which must come together to ensure the delivery of HIGH QUALITY CARE: Effectiveness of the treatment and care provided to patients – measured by clinical outcomes and patient related outcomes The Safety of treatment and care provided to patients The experience patients have of the treatment and care they receive (Lord Darzi, NHS Next Stage Review, Leading Local Change, May 2008.) The NHS Constitution (2010) enshrines the right of people to receive high quality care and treatment
History of Clinical Governance 1997 : Labour Government in the White Paper ‘The New NHS’ – Modern & Dependable abandoned the internal market and introduced a statutory duty for quality improvement that was called CLINICAL GOVERNANCE. 1999: Trust Boards assumed a legal responsibility for quality of care that is equal in measure to their other statutory duties. Clinical governance is the mechanism by which that responsibility is discharged 2003: This “Duty of Quality” is a legal requirement and is found in the Health and Social Care (Community Health and Standards) Act 2003: 2004: Health Commission established to improve the quality of services in the NHS 2009: Department of Health.: A First Class Service 2009: Standards for Better Health Declaration 2009: Care Quality Commission to regulate National Standards across health and social care providers
Service User Involvement The Legislative Framework to ‘put patients at the centre of care’ was announced through the NHS Plan -Section 11 of the Health and Social Care Act 2001; This act came into force on 1st January 2003 and states that all Trust’s must, as a matter of course, consult and involve patients and members of the public; Consult not just when a major change is proposed, but in the on going planning and development and the delivery of services day to day. • Key Components of Clinical Governance • Person centred care with service user involvement Visible Trust Board Level leadership • Use of Clinical Information; • Patient safety and robust risk management; • Clinical Audit; • Research & Development • Clinical Effectiveness • Staffing & Management; • Feedback from Service Users • We must actively seek feedback from our service users and make sure that action and changes occur in response to this feedback. Feedback can come from a variety of sources: • Sources of Feedback • Complaints / compliments; comment cards • National Surveys (including the National Patients Survey); • Local Surveys; • Advocacy services • The Patient Advice and Liaison Service (PALS); • Patient’s experience group (PEx). • Involvement in the annual Business Planning cycle along with staff and other stakeholder groups • Service user son recruitment panels • Staff induction training for staff • Take it to the Top Forums give direct access to the Chief Executive and Team • Mystery Shoppers • Focus Groups
Continue Feedback can come from a variety of sources, including: Advocacy Services Focus Groups Patients Experience Groups (PEx) National Surveys Everything mentioned
Trust Board Leadership Regular visits from executive and non-executive directors to clinical areas to discuss element of quality and safety: Patient safety walk rounds Director CQC spot checks Improvement programmes led by directors and senior management. • PALS Involvement • Patients, relatives or carers may sometimes need help, advice or support; • PALS will provide confidential advice and support, helping with any concerns about the care provided by the Trust; • PALS can guide patients, relatives and carers through the different services available • Use of Clinical Information - Evidence • Clinical Governance requires evidence of effective patient care and safe and appropriate services; Accurate, meaningful and reliable information provides a vital support to quality improvement processes; • Information comes from many different sources including: • Routine monitoring and reports; • Clinical Audit; • Essence of Care Benchmarks • Productive Series outcomes • Patient & Carers surveys • Ward Dashboards
Continue Clinical Governance requires evidence of effective patient care and safe and appropriate services. This evidence can come from: Clinical Audit Ward Dashboards Routine Monitoring and Reports Everything Mentioned
Risk Management • People Safety is about ensuring that people in our care receive high quality care and treatment by the right people at the right time in the right place. • There are risks associated with all episodes of care. • Risk Management is about minimising risks to patients and staff; • It is a positive function and central to the quality of care we give to patients • Risks need to be avoided or controlled; • We do this by carrying out a Risk Assessment and agreeing the level of seriousness attached to each risk; • Actions are then taken on the result of the Risk Assessment to ensure everyone's safety. • Where risks cannot be completely removed we aim to minimise the harm caused by any adverse incidents. • Risk Management is about "stopping bad things from happening" • Clinical Audit • As part of local arrangements for clinical governance, all NHS organisations are required to have a comprehensive programme of quality improvement activity that includes clinicians participating fully in audit; • Clinical audit is the component of clinical governance that offers the greatest potential to assess the quality of care routinely provided for NHS users – audit should therefore be at the very heart of clinical governance systems; • National Institute for Health & Clinical Excellence (NICE). • Clinical Audit is part of the CQUIN and Quality Account work undertaken in local areas in partnership with commissioners
Research & Effectiveness - Evidence Based Practice The work that we carry out daily should be based on accepted good practice. It should be proven to be appropriate and effective by people with knowledge and expertise. This is evidence based practice; The guidance provided by the National Institute for Health & Clinical Excellence (NICE) is a good example of evidence based practice. NICE Guidance NICE develop and distribute guidelines, technology appraisals (Drugs and equipment) and quality standards on a national level. These guidelines are all evidence based and well researched before distribution. Each Trust within the country is responsible for evidencing compliance with the NICE Guidance. The Head of Clinical Effectiveness has responsibility to ensure that we are applying all the NICE guidelines, where appropriate. Local NICE Groups have responsibility to ensure that where guidance is applicable there is an achievable action plan in place monitored within the service and progress sis reported to the Clinical Effectiveness Group (CEG) The Clinical Effectiveness Group (CEG) is responsible for ensuring that key decisions are made in relation to NICE guidelines.
Continue Local NICE Groups have responsibility to ensure that where guidance is applicable there is an achievable action plan in place monitored within the service and progress is reported to the Clinical Effectiveness Group (CEG) True False
Doing things differently If you do what you always did, you get what you always got! • Staffing & Management • The Trust aims to: • have staff that are well trained and have appropriate skills to provide a high quality service through: Training; • Education; • Appraisal; • Clinical & Managerial Supervision • Education & Training • The Trust aims to: • Develop staff, at all levels, to their full potential, as a means of providing high quality, efficient and effective services and individual patient care; • Become a centre of excellence for lifelong learning which is fundamental to the continuous improvement of services to patients and to fulfilling the local and national objectives; • Supporting personal growth, career development and employability, against a background of on going organisational change. Care Quality Commission The purpose of the Care Quality Commission is to promote improvements in the quality of healthcare and public health, through independent, authoritative, patient-centred assessments, of the performance of those who provide services. From 1 April 2009 the Care Quality Commission brought together the Commission for Social Care Inspection, the Healthcare Commission and the MH Act Commission. This now concludes the Clinical Governance section of the training. Please continue to the next section All Trusts are monitored by the Care Quality Commission.
Medicines Management • Target Audience • The target audience for this course includes: • Medical Staff; • Qualified Nursing Staff; • Associate Practitioners; • Clinical Support Workers; • Social Care Staff; • all other SEPT staff with any clinical input • If you are working with medicines on a regular basis you should read Policy CLP13 and Procedural Guideline CLPG13 as soon as possible. This can be found on the intranet (Core services/ Policies and procedures/ Clinical Policies and procedures) • The remainder of these slides briefly summarise major points from CLPG13, but they should not replace reading the original document. You will be expected to know the guidelines as they relate to your role. COURSE OBJECTIVES • Safe and Secure Handling procedures for medicines; • Further training available; • Useful resources relating to medicines
Safe & Secure Handling of Medicines - Prescribing • Only official prescriptions can be used when prescribing: SEPT Drug Prescription and Administration Record (inpatients); • SEPT Outpatient Prescription & Administration Record for Intramuscular Antipsychotic Depot Injections; • SEPT Outpatient Prescription (for medicines to be dispensed "in-house" by the SEPT Essex Pharmacy Departments) e.g. clozapine, alprazolam; • FP10 prescriptions (green prescription pad) for medicines to be dispensed by any community pharmacy in the UK; • Drug and Alcohol FP10 prescriptions for treatment of dependency; • Home Delivery Prescriptions for Risperdal Consta; • In Essex FP10 pads and SEPT Outpatient Prescription pads are available from the Pharmacy Departments at Rochford Hospital and Basildon Mental Health Unit (Level A). Trainee doctors need to present an introductory letter from their consultant when collecting a pad. • In Luton and Bedfordshire follow local procedures to obtain prescription pads (not from pharmacy).
Safe & Secure Handling of Medicines - Verbal Orders and Written Orders • For a new drug with no current prescription – verbal orders are not allowed; • For a dose change of a currently prescribed drug – verbal orders are allowed in exceptional circumstances (fax or e-mail may be used); • If fax / e-mail unavailable, a verbal order may be made by phone, and witnessed by a second nurse; • In an extreme emergency, if there is no current prescription, and the prescriber is genuinely unable to attend the ward, nurses must ask for a WRITTEN, FAXED (not emailed) order from the prescriber. This WRITTEN order, to be signed by the prescriber and faxed to the nurse, must include all the patient's identification, eg DOB, NHS Number etc., and its indication for use; • Both verbal and written orders are only valid for one dose or 24 hours, whichever is the shorter, and must be signed within 24 hours by the prescriber. • Safe & Secure Handling of Medicines - Procurement • Medicines will be supplied by a hospital or community pharmacy; • No samples may be accepted from drug company representatives; • Patient's own drugs can and should be used if checked and approved for use by pharmacy or medical staff. • Safe & Secure Handling of Medicines - Storage • All medicines should be locked away; • Keys must be kept safe; • External and internal medicines should be stored separately; • Medicines requiring a fridge should have a dedicated drugs fridge.
Continue For a new drug with no current prescription… Verbal orders are allowed Verbal orders are not allowed Only verbal orders are allowed
Safe & Secure Handling of Medicines - Administration • Medicines may only be administered by a: Qualified Nurse; • Student Nurse or Student Associate Practitioner, supervised by a qualified nurse; • Associate Practitioner; • Doctor; • Support workers may be delegated the task of medicines administration by the Qualified Nurse in charge. • Social workers may observe patients taking their own medicines, but may not administer them. • The relevant Prescription and Administration Record should be used for all inpatient and community patients. • The Trust administration procedure should be followed –displayed in all clinical areas. • Safe & Secure Handling of Medicines - Transport • Medicines should be transported in sealed containers; • Medicines should follow the patient when moving from one clinical area to another. • Safe & Secure Handling of Medicines - Destruction • Medicines that cannot be re-used (e.g. spoilt doses, unused half-tablets, refused doses already removed from their foil-blister) should be disposed of in the appropriate clinical bin - see your local clinical procedure; • Illicit drugs should be kept in the controlled drug cupboard, details recorded in the ward controlled drug record book, and local procedures followed to dispose of them.
Continue Social Workers may observe patients taking their own medication, and may also administer them True False
Safe & Secure Handling of Medicines – Controlled Drugs • Controlled Drug stocks must be checked weekly; • Leave and discharge prescriptions for Controlled Drugs must have the total quantity written in words and figures. • Safe & Secure Handling of Medicines - Errors • Medicines errors should be reported on a DATIX Form. • It is the responsibility of the person finding the error to report it. Further Training Staff will be asked to attend or complete the following courses: Trainee Doctors: medicines related training during Thursday teaching sessions (Essex) Qualified Nurses: One day course on Medicines Management, every 3 years; E-learning Medicines Calculations and Conversions, every 3 years; Ward or CMHT-based Drug Administration competency assessment, every 3 years. Associate Practitioners: One day course on Introduction to Medicines Management for Associate Practitioners (part of your training); then, one day course on Medicines Management for Associate Practitioners during your training or first year of qualification; then, one day course on Medicines Management, every 3 years (same course as Qualified Nurses); E-learning Medicines Calculations and Conversions, every 3 years; Ward or CMHT-based Drug Administration competency assessment, every 3 years. Support workers, Social Care staff, and any other staff (eg OTs, Psychologists, Counsellors) who handle, manage or discuss medicines with service users: Two hour course on Medicines Management, every 3 years;
Continue Controlled drug stocks must be checked… Monthly Weekly Yearly
Useful Resources • Additional resources you may find useful are: • Medicines Management resources on the Intranet (Library/ Medicines Management) • SEPT Formulary and Prescribing Guidelines, available on the Trust Intranet (Library/ Medicines Management/ Formulary and Prescribing Guidelines) • Pharmacy Telephone Numbers (Essex):Basildon - 01268 243576 • Rochford - 01702 538100 • Pharmacy Department, Bedford Hospital: 01234 355122 ext 6082 • Pharmacy Department, Luton & Dunstable Hospital: 01582 718312 • All staff should read the Safe and Secure Management of Medicines policy and procedures CLP13 and CLPG13. This can be found on the intranet (Core services/ Policies and procedures/ Clinical Policies and procedures) This now completes the Medicines Management section of the training. Please continue to the next section.
Supervision COURSE OBJECTIVES • Be able to define the concept of supervision; • Have an awareness of the importance of supervision, in relation to supporting staff and providing high quality services; • Be able to differentiate between Clinical supervision and Managerial supervision; • Have an understanding of the process / formation of supervision. Supervision Policy Are you aware there is a supervision policy? There is! SEPT has made a big commitment to ensuring that every employee in this Trust will be afforded the time for supervision, regardless of the environment they are working in or status. Therefore the contents of this module reflect the policy guidelines that represent your area. In order to ensure supervision takes place, the Trust undertakes an annual audit, as evidence it demonstrates its commitment to supervision. On analysis of the audit, any improvements required are implemented and the policy is updated. • The Aim of Supervision • It enables supervisees to: • Achieve; • Sustain; • Creatively develop a high quality practice, through the means of focussed support and development ( As directed by the Nursing & Midwifery Council (NMC)). • Supervision is not 'Big Brother' watching you, but about supporting you in your day-to-day job, with patients, and your personal development. The benefits of supervision are countless, so it is around to stay and isn't optional!
Supervision Components There are two components to supervision: Clinical supervision Managerial supervision In addition to the above two forms of supervision, one can have the option of peer supervision or professional supervision, dependant on your service focus. • Clinical Supervision • Clinical Supervision is a primary source of support, which brings practitioners and skilled supervisors together to: • Reflect on practice; • Identify areas of improvement; • Enable the maintenance and development of high quality clinical care. • All professional groups are required to undertake supervision in accordance with the code of practise. • Supervision is important because it allows an individual the opportunity, with their supervisor, to discuss key clinical issues, in terms of client / patient care, and issues pertaining to specific individual clinical problems. • For example ... A patient has recently been admitted with Huntington's Chorea and is problematic. What management approaches would you use and what research has been undertaken, in the clinical management of this type of patient, are good examples of an issue to discuss in clinical supervision.
Continue As well as the two components of supervision, clinical supervision and managerial supervision, there is also the option of peer supervision and professional supervision, depending on your service focus. True False
Managerial Supervision • Managerial Supervision is designated time with your line manager to: • Discuss; • Reflect; • Identify areas of your workload which focuses on: • Management issues • Personal training • Development • Is this different to an appraisal? Yes, because an appraisal is an annual review of your personal development. Where as managerial supervision is focussing on the day-to-day work load issues, which may form part of your appraisal in terms of your personal development. • For example ... As part of your role on the ward or department, you have been tasked with undertaking group work. You have learnt some of the skills for facilitation of group work, but you are experiencing difficulties and feel that this is an area you would like to pursue and need further training in. Although this is discussed in supervision, there will be an opportunity for addressing this in your annual appraisal review, as part of your development. Who is supervision for? For all health and social staff: Qualified; Unqualified; All professional / non professional groups.
Continue Managerial Supervision is different to an appraisal? Yes – An appraisal is an annual review of your development, not focussing day to day workload issues No – The two are interchangeable. You don’t need to do both
Can I choose my supervisor? Yes, if it is for clinical supervision, which can be undertaken by a colleague, within the organisation. However if you are a professional with specific needs, such as a Family Therapist, Psychologist or other, and there are no staff with such expertise in the organisation, then you may seek external supervision. As this is a professional service, there is a cost implication, which must be pre-approved by your line manager. How much supervision must I have? As a minimum, all staff must receive managerial supervision on a regular basis. Although there is no hard and fast rule to this, we would advise you allow a minimum of 30 minutes and a maximum of 2 hours, dependant on your individual needs and circumstances. However this will vary with different professional groups and service areas. Each professional group must follow the supervision policy, as per their professional guidelines. Although, note, the policy states that supervision must be undertaken, as a minimum, at least 8 times a year. Who's Responsibility Is It? It is the line manager's responsibility to ensure that their members of staff receive regular supervision, in accordance with the supervision policy and guidelines. It is also the responsibility of the individual to ensure that they receive regular supervision. If supervision is not taking place, due to various reasons, it is the individual's responsibility to ensure that they bring this to the manager's attention and it is the manager's responsibility to provide commitment to supervision (e.g. reschedule the meeting). If supervision is continually cancelled, you have a duty, as an individual, to raise this with your line manager's manager
Continue Supervision must be undertaken at least how many times a year? 4 16 0 8
Is Supervision Confidential? Yes. Confidentiality must be observed throughout the whole process. All meetings are confidential unless there is a need to disclose serious concerns on your part, issues of misconduct, poor or unsafe practice. • Supervision Format • The format / structure for supervision is: • Guaranteed time / protected time; • Confidential environment; • Confidential records by supervisor / supervisee, with an action plan; • Supervision contract (frequency, timing, location, an agenda); • Agenda to reflect discussion; • Two way reflective discussion. • By having a structure you ensure a dedicated time, the full attention of your manager and safety to discuss any issues, in a confidential setting and away from your working environment (e.g. office / meeting room). This now completes the Supervision section of the training. Please continue to the next section.
NHS Protect ~ Security Management COURSE OBJECTIVES • NHS Protect background • NHS Protect role • What security management means • The role of the Trust LSMS • Related Policies • Violence and aggression • De-escalation Background In April 2011 the NHS Security Management Service was reviewed as part of a national review of government funded bodies and is now known as NHS Protect. The Role of NHS Protect NHS Protect has overall responsibility for all policy and operational matters, related to the management of Security within the NHS. NHS Protect leads on work to identify and tackle crime across the health service. The aim is to protect NHS staff and resources from activities that would otherwise undermine their effectiveness and their ability to meet the needs of patients and professionals. Ultimately, this helps to ensure the proper use of valuable NHS resources and a safer, more secure environment in which to deliver and receive care.
NHS Protect Structure • NHS Protect has been reorganised to have three distinct service areas: • Policy guidance for the NHS • 2. Deterrence of crime, violence and fraud in the NHS • 3. Operational security management and counter fraud services: • Local support and development services (to support LSMS’s and their NHS Trust) • National investigation services • Information and intelligence services • NHS Protect works closely with the Health & Safety Executive and the CQC in monitoring the required security management standards in NHS Trusts.
The Local Security Management Specialist • As an organisation we have appointed an Accredited Local Security Management Specialist (LSMS), whose role is to implement the national security management strategy and guidance at SEPT. • LSMS work takes place within a clear legal framework, set out in Directions issued by the Department of Health to relevant health bodies and the strategic framework outlined in the National Strategy document. • Only the LSMS may perform the duties and functions described in Directions, subsequent guidance and requirements specified in the NHS Security Management Manual. • The LSMS leads, assists in and co-ordinates the prevention strategies, investigation of all assaults and other criminal activity and resultant actions at SEPT. • The LSMS is the central contact point for NHS Protect, and will facilitate information sharing and gathering between SEPT and NHS Protect, including Safety Alerts and annual statistics relating to assaults within the organisation.
Continue The LSMS is the central contact point for NHS protect, and will facilitate information sharing and gathering between SEPT and NHS Protect. True False
The Local Security Management Specialist • The LSMS is the central contact point for the police and staff within SEPT when dealing with assaults and other criminal acts under investigation. • Currently your LSMS's for Mental Health & Learning Disability Services and Community Health Services are based in the Risk Management Department in Essex, details of which can be found in the intranet. • Our Non-Executive Director ensures and monitors necessary requirements are in place within the Trust and guidelines adhered to. • The Trust’s Director nominated as the 'Security Management Director' (SMD) has overall responsibility for security management work with particular responsibilities for tackling violence within SEPT.
NHS Protect Violence Strategy • NHS Protect is committed to tackling violence towards NHS staff. It strives to ensure strategies are developed and put in place to promote safer work environments for these staff. This is supported by Policy on Violence & Aggression at Work. • NHS Protect also recognises that staff working in certain settings have specific and complex needs. An example is mental health or learning disabilities settings, where there are higher levels of violence. Violence within these settings can be attributed to a range of factors, including environmental and cultural ones. • Secretary of State Directions state that all NHS front line staff must be trained in Conflict Resolution Training and in Mental Health & Learning Disability services a specific Promoting Safe & Therapeutic Services (PSTS), both are an integral part of the violence strategy and NHS Trusts are required to submit their training figures every year. • SEPT has incorporated this national guidance into its Prevention & Management of Violence & Aggression (PMVA) Policy and Procedural Guidelines (RM05) and provides a range of PMVA training based on staff role.
Property & Assets • NHS Protect works to protect and secure NHS property and assets. • Assets can be defined as ‘the materials and equipment used to deliver NHS healthcare. In respect of staff, professionals and patients it can also mean the personal possessions they retain whilst working in, using or providing services to the NHS’.
Property & Assets NHS Protect is undertaking work in the following areas: • Ensuring the security of all NHS property and assets, regardless of type, size or value; • Joint work with the Home Office to make all NHS car parks safe; • Secure by Design – work to explore ways in which security can be ‘designed in’ at planning stage for new builds and refurbishment in the NHS. • Lockdown Guidance and training to enable Trusts to deliver robust Lockdown policies, procedures and local plans.
Counter Terrorism • In response to the terrorist threat, NHS Protect is committed to working with national, regional and local stakeholders to ensure that all Trusts identify vulnerability and adopt risk-assessed proportionate protective security measures. • NHS Protect provides guidance and support to LSMS's to deliver the 'Protect' strand of 'Contest' - which is the Governments national counter - terrorism strategy: • CONTEST is organised around four principal work streams: • Pursue: to stop terrorist attacks • Prevent: to stop people from becoming terrorists or supporting terrorism • Protect: to strengthen our protection against terrorist attack • Prepare: where an attack cannot be stopped, to mitigate its impact • SEPT has policies for Management of Security (RM09) and specific guidance for managing a Bomb Threat or Hoax (Appendix RMPG09b)
NHS Protect Legal Protection Unit (LPU) • The NHS Protect Legal Protection Unit (LPU) works closely with the following bodies to safeguard NHS staff and assets from violent and disruptive individuals: • The police • The Crown Prosecution Service • Local authorities • Health bodies. • It does this by providing advice and assistance on a wide variety of issues and, in appropriate cases, commencing legal proceedings. The LPU can take action in the civil courts to obtain injunctions, and can also seek antisocial behaviour orders. • Where appropriate, the LPU, in conjunction with NHS Trusts, will prosecute individuals who have assaulted or abused NHS staff, in cases that have not been progressed by the police or the Crown Prosecution Service. This approach has led to the successful prosecution of a number of individuals who would otherwise have escaped justice.
NHS Protect Legal Protection Unit (LPU) • The LPU assists NHS Trusts with: • Legal advice on issues such as withholding treatment • Legal advice on the most appropriate sanctions available for specific cases • Legal advice on the most appropriate redress available for specific cases • Legal advice in cases of physical and non-physical assault • Drafting warning letters and acknowledgement of responsibilities agreements. • Area Security Management Specialist's • NHS Protect employs regional Area Security Management Specialists who provide operational support to the network of Local Security Management Specialists. • Area Security Management Specialists (ASMSs) provide the link between the network of Local Security Management Specialists and NHS Protect, ensuring that operational work informs and drives revision of national policy, systems and procedures. • The ASMS’s manage the regional Local Security Management Specialist networks, ensuring that best practice is highlighted and that updated legal and procedural information is made available.
Security at SEPT • SEPT has a legal responsibility to provide a safe and secure environment for staff, service users and visitors. • SEPT employees also have a responsibility to ensure that both their personal property and Trust property and assets they have access to are managed securely. • All security related incidents must be reported on Datix. If you identify any security risks or issues, you must discuss with your line manager and/or contact the LSMS for advice. • There is a comprehensive Management of Security Policy and Procedural Guideline in the policy library (RM09) which can be found in the Risk Management Policy Folder on the SEPT Intranet.
Lone working NHS Protect defines lone working as: 'any situation or location in which someone works without a colleague nearby; or when someone is working out of sight or earshot of another colleague‘ The Health and Safety Executive (HSE) defines lone workers as: 'those who work by themselves without close or direct supervision' A Lone Worker is a member of Trust staff who works, either regularly or only occasionally, on their own, and without access to immediate support from managers or other colleagues. This could be outside of a hospital or similar environment or internally. Lone Working may be a part of a person’s usual role or it could occur on an infrequent basis. Lone Working is not unique to any particular groups of staff, working environment or time of day. There is not one single definition that encompasses all those who may face lone working situations and, therefore, may face increased risks to their security and safety. All lone worker staff must have a risk assessment undertaken by their line manager to ensure that suitable and sufficient control measures are in place The Trust Lone Worker Policy & Procedural Guidelines (CLP38) can be found on the SEPT Intranet. The LSMS manages the NHS Lone Worker Service (lone worker devices) at SEPT.
Definitions of Violence The HSE (1997) describe physical assault and non-physical assault as: Physical Assault - The intentional application of force to the person or another, without lawful justification, resulting in physical injury or personal discomfort. Non-physical Assault - The use of inappropriate words or behaviour causing distress and / or constituting harassment. • The Public Health Model • This model is advocated by the World Health Organisation as the cornerstone of attempts to address workplace violence views prevention as having three dimensions. Each dimension is important but the emphasis is on primary prevention. • The model is shown below: • Primary prevention - preventing violence before it happened by addressing root causes • Secondary prevention - reactive responses de-escalation • Tertiary prevention - physical interventions post incident reviews and debriefs • Prevention at every level of the model requires: • Action at the level of the organisation • The staff team • The individual worker • The service user
Continue The HSE describe which type of assault with the following definition: ‘The intentional application of force to the person or another, without lawful justification, resulting in physical injury or personal discomfort’ Physical Assault Non-Physical Assault
First Line Intervention To de-escalate a developing situation, verbally is clinically ethically and legally preferable to using physical restraint. De-escalatory procedures should therefore be utilised in any arena that requires workers to come into contact with a potentially violent individual. Triggers, Weapons & Targets Triggers Triggers of violence and aggression are: Verbal - phrases which evoke anger / frustration; Physical - causing pain / discomfort, touch, invading personal space, poor use of body language; Environmental - noisy surroundings, lack of privacy, peer pressure towards anti-social behaviours. The above may sometimes involve causing offence to an individual on the grounds of their sexuality, culture of spiritual beliefs, or just unluckily pressing the wrong button(s). Weapons Some body parts may be used as a weapon, where inanimate objects are concerned. Targets The recipient of the assailant's aggression. • Circles of Influence • This concept is relatively simple. There are certain things that we have significant control over, notably our own non-verbal and verbal behaviour. There are other factors that are role dependant, which we may have less control over, such as the behaviour of other members of staff (although there is a responsibility to report abuse). • Commonly reported reactions to violence and fear and / or frustration and anger. Unless all three are acknowledged and managed, it can: • Diminish cognitive control • Evoke your own fight or flight reaction • Promote a desire to punish the service user for making us feel like this
Counter Aggression Counter aggression, in a care setting, is inappropriate. At times an assertive response may be necessary and warranted, but not an aggressive one. Staff have a responsibility to recognise and manage their own emotions and monitor the emotions of other staff, involved in a situation, to ensure safety of all • Managing your Emotions • Recognise and acknowledge signs of anxiety; • Recognise danger signals of your own and others' anger; • Take one deeper, than normal, breath and exhale slowly; • Use positive self statements (e.g. I can cope); • Focus on active listening; • Avoid a defend-attack spiral; • Choose what you are going to do • Violent Incident Models • There are five possible incident models; the underlying idea is that each incident is a unique event. However there may be common patterns amongst types of incidents. If staff can learn to recognise incident types, then they can adapt their response accordingly. • The five possibilities are: • Affective • Instrumental • Mixed • Aversive • Stimulus - Response – Consequence
Continue When managing our emotions we should try to… Recognise and acknowledge signs of anxiety Focus on active listening Use positive self statements Take one deeper than normal breath and exhale slowly Everything mentioned
Non-verbal De-escalation Verbal de-escalation is a skilled intervention, that is specifically used to intervene, when a patient's behaviour moves from being normal, for that individual, to a state that can be recognised as pre-aggressive. The technique particularly lends itself to use by health care workers, who spend long periods of time with patients, have formed a relationship and can note the early warning. It is important to appreciate and attend to our and others non-verbal behaviours and the need for cultural sensitivity. For example, in Iranian communities, thumbs-up, which indicates good in many western societies, is generally considered very rude. Any response to a potential incident must be guided in the first instance with an awareness of the risk the situation presents. The options are to stay or to leave the situation.