Download

1 / 33
370 likes | 430 Views
Nasopharyngeal Angiofibroma :. Juvenile Nasopharyngeal Angiofibroma (JNA) highly vascular benign yet unencapsulated tumor of adolescent males. Frequency: JNA accounts for 0.05% of all head and neck tumors. Sex: JNA occurs exclusively in males.

E N D
Nasopharyngeal Angiofibroma: • Juvenile Nasopharyngeal Angiofibroma (JNA) • highly vascular benign yet unencapsulated tumor of adolescent males.
Frequency: JNA accounts for 0.05% of all head and neck tumors. • Sex: JNA occurs exclusively in males. • Age: range is 7-19 years. JNA is rare in patients older than 25 years • Etiology: A hormonal theory has been suggested due to the lesion's occurrence in adolescent males.
Pathophysiology: The tumor starts adjacent to the sphenopalatine foramen. Large tumors frequently are bilobed or dumbbell-shaped, with one portion of the tumor filling the nasopharynx and the other portion extending to the pterygopalatine fossa.
Clinical: Symptoms: • Nasal obstruction (80-90%): • Epistaxis (45-60%): • Headache (25%): • Facial swelling (10-18%) • Other symptoms include unilateral rhinorrhea, anosmia, hyposmia, rhinolalia, deafness, otalgia, swelling of the palate, and deformity of the cheek.
Signs: • Nasal mass (80%) • Orbital mass (15%) • Proptosis (10-15%) • Other signs may include -Serous otitis due to eustachian tube blockage. -Zygomatic swelling and trismus denote spread of the tumor to the infratemporal fossa.
Differentials: • Other causes of nasal obstruction, (eg, nasal polyps, antrochoanal polyp, teratoma, encephalocele, dermoids, inverting papilloma, rhabdomyosarcoma, squamous cell carcinoma) • Other causes of epistaxis, systemic or local • Other causes of proptosis or orbital swelling
Medical therapy: • Surgical therapy • Hormonal therapy • Radiotherapy Biopsy is prohibited because of severe bleeding
Nasopharyngeal malignancies • Nasopharyngeal carcinoma (NPC) • Lymphoma • Salivary gland tumors • Sarcomas
Nasopharyngeal Carcinoma More common in Asia
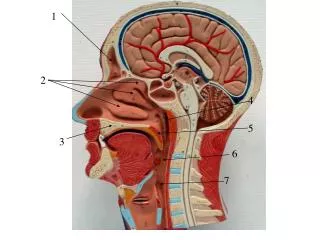
Anatomy • Anteriorly -- nasal cavity • Posteriorly -- skull base and vertebral bodies • Inferiorly -- oropharynx and soft palate • Laterally -- • Eustachian tubes and tori • Fossa of Rosenmuller - most common location
Anatomy • Close association with skull base foramen • Mucosa • Epithelium - tissue of origin of NPC • Stratified squamous epithelium • Pseudostratified columnar epithelium • Salivary, Lymphoid structures
Epidemiology • Chinese native (广东,广西。湖南,福建) • > Chinese immigrant > North American nativeBoth genetic and environmental factors • Genetic • HLA histocompatibility loci possible markers
Epidemiology • Environmental • Viruses • EBV- well documented viral “fingerprints” in tumor cells and also anti-EBV serologies with WHO type II and III NPC • HPV - possible factor in WHO type I lesions • Nitrosamines - salted fish • Others - chronic nasal infection, poor hygiene, poor ventilation
Clinical Presentation • Often subtle initial symptoms 1. unilateral HL (SOM) 2. epistaxis 3. painless, slowly enlarging neck mass Larger lesions 4. nasal obstruction 5. cranial nerve involvement
Clinical Presentation • Xerophthalmia - greater sup. petrosal n • Facial pain - Trigeminal n. • Diplopia - CN VI • Ophthalmoplegia - CN III, IV, and VI • cavernous sinus or superior orbital fissure • Horner’s syndrome - cervical sympathetics • CN’s IX, X, XI, XII - extensive skull base
Clinical Presentation • Nasopharyngeal examination • Fossa of Rosenmuller most common location
Regional spread • Usually ipsilateral first but bilateral not uncommon • Distant spread - rare (<3%), lungs, liver, bones
Radiological evaluation • Contrast CT with bone and soft tissue windows • imaging tool of choice for NPC • MRI • soft tissue involvement, recurrences • Chest CT, bone scans
TNM classification • Class 0: Tis N0 M0 • Class I: T1 N0 M0 • Class II A: T2a N0 M0 • Class II B: T1 N1 M0 ; T2a N1 M0 ; T2b N0, N1 M0 • Class III: T1 N2 M0 ; T2a, T2b N1 M0 ; T3 N0, N1, N2 M0
Class IV A: T4 N0, N1, N2 M0 • Class IV B: any T N3 M0 • Class IV C: any T any NM1
Treatment • External beam radiation • Dose: 6500-7000 cGy • Adjuvant brachytherapy • mainly for residual/recurrent disease
TreatmentSurgical management • Mainly diagnostic - Biopsy • Surgical treatment • primary lesion • regional failure with local control
TreatmentSurgical management • Primary lesion • consider for residual or recurrent disease • approaches • infratemporal fossa • transparotid temporal bone approach • transmaxillary • transmandibular • transpalatal
TreatmentSurgical management • Regional disease • Neck dissection may offer improved survival compared to repeat radiation of the neck
Treatment • Chemotherapy • Immunotherapy
Congenital tonsillar masses • Teratoma • Hemangioma • Lymphangioma • Cystic hygroma
Treatment: • Laser therapy • Surgery
Malignant Neoplasms • Most common is lymphoma • Non-Hodgkin’s lymphoma • Rapid unilateral tonsillar enlargement associated with cervical lymphadenopathy and systemic symptoms
Treatment • Radiotherapy and chemical therapy



![Nasopharyngeal Cancer [6]](https://cdn1.slideserve.com/3354426/nasopharyngeal-cancer-6-dt.jpg)