Download
1 / 31
340 likes | 514 Views
Clinical Efficacy of Clopidogrel in CVA, ACS, PAD. Atherothrombosis: A Generalized and Progressive Process. Unstable angina MI Ischemic stroke/TIA Critical leg ischemia Cardiovasculardeath. ACS. Atherosclerosis. Atherothrombosis. Stable angina Intermittent claudication.

E N D
Atherothrombosis: A Generalized and Progressive Process Unstable angina MI Ischemic stroke/TIA Critical leg ischemia Cardiovasculardeath ACS Atherosclerosis Atherothrombosis Stable angina Intermittent claudication Adapted from Stary HC et al. Circulation. 1995; 92: 1355–74, and Fuster V et al. Vasc Med. 1998; 3: 231–9.
Collagen thrombin TXA 2 TXA 2 Synergistic Mode of Action with Clopidogrel and ASA1 CLOPIDOGREL C ADP ADP GPllb/llla (Fibrinogen receptor) Activation ASA COX ASA COX (cyclo-oxygenase) ADP (adenosine diphosphate) TXA2 (thromboxane A2) 1. Schafer AI. Am J Med 1996; 101: 199–209.
16 12 8 4 0 CAPRIE: Long-Term Benefit of Clopidogrel Compared with ASA1 Cumulative Event Rate (Myocardial Infarction, Ischemic Stroke or Vascular Death) 8.7%*Overallrelativeriskreduction ASA Clopidogrel Cumulative event rate (%) p = 0.043, n = 19,185 0 3 6 9 12 15 18 21 24 27 30 33 36 Months of follow-up *ITT analysis 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329–39.
ASA 19.2%*Relativeriskreduction 5 ASA 3.6% Clopidogrel 4 3 Cumulative event rate (%) Clopidogrel 2.9% 2 1 p = 0.008, n = 19,185 0 0 3 6 9 12 15 18 21 24 27 30 33 36 CAPRIE: Benefit of Clopidogrel over ASA in the Reduction of Myocardial Infarction1 Months of follow-up *ITT analysis 1. Gent M. Circulation 1997; 96(suppl 8): I-467.
30% 34* 28* 23.8% 25% 20.4% 11* 20.0% ASA 20% 17.2% 15.2% Clopidogrel 14.1% Event rate (%) 15% 10% 5% 0 All CAPRIE patients†1 Prior history of any Prior history of major (n = 19,185) ischemic event‡2 acute event (MI or stroke)‡2 (n = 8,854) (n = 4,496) CAPRIE: Amplified Benefit of Clopidogrel in Patients with Higher Vascular Risk Event Rate(Myocardial Infarction, Ischemic Stroke, or Vascular Death) *Number of events prevented/1,000 patients/year over ASA †Cumulative proportion of patients experiencing event over 3 years (mean follow-up, 2 years) ‡3-year event rate 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329–39. 2. Jarvis B, Simpson K. Drugs2000; 60: 347–77.
38† 21.5% 21† 20% 17.7% 17.7% 11† 15.6% 13.7% 15% ASA 12.6% Annual event rate (%) Clopidogrel 10% 5% 0 All CAPRIE patients¹ Diabetes² Diabetes treated with insulin² CAPRIE: Amplified Benefit of Clopidogrel in Patients with Diabetes Event Rate(Myocardial Infarction, Stroke, Vascular Death, or Hospitalization*) 25% *For ischemic events or bleeding†Number of events prevented/1,000 patients/year over ASA 1. Bhatt DL et al. Am Heart J 2000; 140: 67–73. 2. Jarvis B, Simpson K. Drugs 2000; 60: 347–77.
25% 22.3% 64† 20% 11† 15.9% 13.7% 15% ASA 12.6% Annual event rate (%) Clopidogrel 10% 5% 0 All CAPRIE Prior CABG Overall benefit: p = 0.001; multivariate analysis CAPRIE: Amplified Benefit of Clopidogrelin Patients with Prior CABG1 Event Rate(Myocardial Infarction, Stroke, Vascular Death, or Hospitalization*) *For ischemic events or bleeding†Number of events prevented/1,000 patients/year over ASA 1. Bhatt DL et al. J Am Coll Cardiol 2000; 35(suppl A): 383.
ASA(n = 9,586) Clopidogrel(n = 9,599) p value Adverse experiences† Diarrhea (severe)1Gastritis2Gastro-intestinal ulcer2Gastro-intestinal hemorrhage(severe)1 Intracranial hemorrhage1 Rash (severe)1 Neutropenia2 0.11%1.32%1.15%0.71% 0.49% 0.10% 0.17% 0.23%0.75%0.68%0.49% 0.35% 0.26% 0.10% NS< 0.001 0.001< 0.05 NS < 0.05 NS CAPRIE: Favorable Safety for Clopidogrel Compared ASA* *Patients with ASA intolerance were excluded †Clinically severe or resulting in early drug discontinuation 1.CAPRIE Steering Committee. Lancet 1996; 348: 1329–39. 2. Harker LA et al. Drug Safety 1999; 21: 325–35.
CURE: Design1 Clopidogrel 300mg loadingdose n = 12,562 28 countries Clopidogrel75mg o.d.(n = 6,259) ASA 75–325 mg o.d. Patients with acute coronarysyndrome R Double-blind treatment up to 12 months (unstable angina or non-Q-wavemyocardial infarction) ASA 75–325 mg o.d. Placebo 1 tab o.d.(n = 6,303) Day 1 12 monthor final visit 1 month visit 3 month visit 6 month visit 9 month visit Placebo loading dose Discharge visit R = Randomization 1. The CURE Study Investigators. Eur Heart J 2000; 21: 2033–41.
0.14 Placebo*(n = 6,303) 0.12 0.10 Clopidogrel*(n = 6,259) 0.08 20% Relativerisk reduction p = 0.00009 Cummulative hazard rate 0.06 0.04 0.02 0.00 0 3 6 9 12 Months of follow-up CURE: Early and Long-Term Benefits of Clopidogrel1,2 Cumulative Events (Myocardial Infarction, Stroke, or Cardiovascular Death) *On top of standard therapy (including ASA) 1. The CURE Trial Investigators.N Engl J Med 2001; 345: 494–502. 2. Data on file, 2002, p73 internal CSR-EFC 3307.
0.15 Placebo*(n = 1,345) Median time to PCI 0.10 Clopidogrel*(n = 1,313) Cumulative hazard rate 31% Relativerisk reduction p < 0.002 0.05 0.00 10 0 100 200 300 400 Days of follow-up PCI-CURE: 31% Relative Risk Reduction at Long-Term1 Endpoint: Myocardial Infarction or Vascular Death *On top of standard therapy (including ASA) 1. Mehta SR et al.Lancet 2001; 358: 527–33.
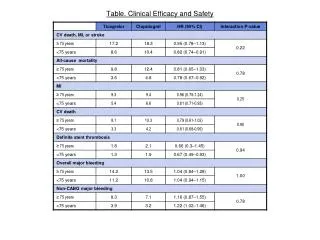
Placebo*(n = 6,303) Clopidogrel*(n = 6,259) Event p value • Major bleeding1 • Life-threatening • Other major bleeding • Transfusions of 2 units of blood1 • Minor bleeding1 • Major bleeding byTIMI definition2 • Major bleeding byGUSTO definition3 2.7% 1.8% 0.9% 2.2% 2.4% 1.2% 1.1% 3.7% 2.2% 1.5% 2.8% 5.1% 1.1% 1.2% 0.001 NS 0.002 0.02 < 0.001 0.70 0.48 CURE: Bleeding Episodes *On top of standard therapy (including ASA) 1. The CURE Trial Investigators. N Engl J Med 2001; 345: 494–502. 2. Chesebro JH et al. Circulation 1987; 76: 142–54. 3. The GUSTO Investigators. N Engl J Med 1993; 329: 673–82.
CURE: Relation Between Safety and ASA Dosage1 6.0% 4.9% 5.0% 4.0% 4.0% 3.5% Bleeding rate (%) 3.0% 2.6% Placebo* 2.3% 2.0% Clopidogrel* 2.0% 1.0% 0.0% < 100 mg 100–200 mg > 200 mg ASA dose 75–325 mg *On top of standard therapy (including ASA) 1. Clopidogrel Prescribing Information, US, February 2002.
ACC/AHA 2002 Guidelines Update for UA and NSTEMI1 Class I Recommendations for Long Term Therapy* ASA† + Clopidogrel†‡ for 9 months + Beta-blockers† + Lipid lowering therapy + ACE I *At hospital discharge and post-hospital discharge†In the absence of contraindications ‡Clopidogrel should be administered to hospitalized patients who are unable to take ASA because of hypersensitivity or major GI intolerance 1. Braunwald E et al. American College of Cardiology (ACC) and the American Heart Association (AHA) Guidelines, USA: ACC/AHA; 2002.
From CAPRIE to CURE – Conclusions • In CAPRIE, clopidogrel was more effective than ASA in reducing the combined risk of myocardial infarction, ischemic stroke, or vascular death1 • Synergistic effects of clopidogrel and ASA have been demonstrated in ex vivo platelet studies and animal models2–5 • Clopidogrel on top of standard therapy (including ASA) demonstrates an early effect (within hours) and sustained long-term benefit throughout the entire 12 month study period in the CURE study:6 • a 20% relative risk reduction in ischemic events with long-term use(up to 12 months) (p = 0.00009)7 • the Kaplan-Meier curves began to diverge within hours and continued to diverge over the 12-month period 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329–39. 2. Cadroy Y et al. Circulation 2000; 101: 2823–8. 3. Herbert JM et al. Thromb Haemost 1998; 80: 512–8. 4. Harker LA et al. Circulation 1998; 98: 2461–9. 5. Makkar RR et al. Eur Heart J 1998; 19: 1538–46. 6. The CURE Trial Investigators. N Engl J Med 2001; 345: 494–502. 7. Data on file, 2002, p73internal CSR-EFC 3307.
סל הבריאות 2006 • המטופל אינו יכול להשתמש באספירין בשל רגישות יתר או כל הוריית נגד אחרת • המטופל פיתח תופעות לוואי לטיפול באספירין • לאחר צינתור לב טיפולי במשך 3 חודשים • בחולים עם תסמונת כלילית חדה שלא ניתן לבצע בהם צנתור כלילי או שמחלתם אינה ניתנת לטיפול על ידי צנתור כלילי טיפולי ( למשך 3 חודשים) • לחולים שלקו בשבץ מוחי שני תוך כדי טיפול מונע באספירין
What is PAD? PAD is an atherothrombotic disorder affecting the peripheral arteries and it is associated with a high risk of MI, stroke and vascular death1 The major risk factors for PAD are:2 • smoking • diabetes • age >55 years (men) or >65 years (women) • hyperlipidemia • hypertension • history of cardiovascular disease 1. Hiatt WR. J Vasc Surg. 2002; 36:1283-1291. 2. Belch JJ et al. Arch Intern Med 2003; 163: 884-892.
Only 1 in 10 patients with PAD has classical symptoms of intermittent claudication 1 in 5 people over 65 has PAD† Only 1 in 10 of these patients has classical symptoms of intermittent claudication (IC) † ABI<0.9 Diehm C et al. Atherosclerosis 2004; 172; 95-105.
Platelet thrombus Platelets adhering to subendothelial space Platelets Endothelial cells Subendothelial space Plateletsare activated following the rupture of an atherosclerotic plaque Normal platelets Activated platelets Platelet aggregation Adapted from: Ferguson JJ. The Physiology of Normal Platelet Function. In: Ferguson JJ. Chronos N, Harrington RA (Eds). Antiplatelet Therapy in Clinical Practice. London: Martin Dunitz; 2000: 15–35.
Prevalence of PAD increases with age Rotterdam Study (ABI Test <0.9)1San Diego Study (PAD by noninvasive tests)2 Patients with PAD (%) Figure adapted from Creager M, ed. Management of Peripheral Arterial Disease. Medical, Surgical and Interventional Aspects. 2000. 1 Meijer WT et al. Arterioscler Thromb Vasc Biol 1998; 18: 185-192. 2.Criqui MH et al. Circulation 1985; 71: 510-515.
Measuring Ankle-Brachial Index (ABI) Video courtesy of Professor Curt Diehm, Karlsbad-Clinic, Academic Teaching Hospital of the University of Heidelberg, Germany.
Association of low ankle brachial index with highmortality in primary care European Heart Journal (2006) 27, 1743–1749
Ankle systolic pressure Brachial systolic pressure How is Ankle-Brachial Index (ABI) measured? ABI = • Measure ankle and brachial systolic pressures with Doppler1,2 • Use highest arm and each ankle pressures1,2 ABI Interpretation3 > 0.90 Normal 0.41 – 0.90 Mild-to-moderate peripheral arterial disease 0.00 – 0.40 Severe peripheral arterial disease 1. TASC Working Group. Int Angiol 2000; 19 (suppl): 5-34. 2. Vascular Disease Foundation, 2003. Available at:http://www.vdf.org/ABI.htm. 3. Hiatt WR. N Engl J Med 2001; 344: 1608-1621.
There is a strong two way association between decreased ABI and increased risk for cardiovascular death1 70 60 All-cause mortality CVD mortality 50 40 Percent (%) 30 20 10 0 <0.60 (n=25) 1.0-<1.10 (n=980) 0.90-<1.0 (n=195) 0.60-<0.70 (n=21) 0.70-<0.80 (n=40) 0.80-<0.90 (n=130) Baseline ABI* *Mean participant follow-up 8.3 years Resnick HE et al. Circulation 2004; 109: 733-739.
Patients with PAD are at high risk of MI and stroke * Over 10 years versus the general population except for stroke following stroke which measures subsequent risk per year † Sudden death defined as death documented within 1 hour and attributed to coronary heart disease. 1. Adult Treatment Panel II. Circulation 1994; 89: 1333-1435. 2. Kannel WB. J Cardiovasc Risk 1994; 1: 333-339. 3. Wilterdink JI, Easton JD. Arch Neurol 1992; 49: 857-863. 4. Criqui MH et al. N Engl J Med 1992; 326: 381-386.
Risk of death is increased in patients with both symptomatic and asymptomatic PAD 100 Normal subjects* 75 Asymptomatic PAD† 50 Survival (% of patients) Symptomatic PAD† 25 Severe symptomatic PAD† 0 0 2 4 6 8 10 12 Year *Kaplan-Meier survival curves based on mortality from all causes.†Large-vessel PAD. Criqui MH et al. N Engl J Med 1992; 326: 381-386.
The American Diabetes Association recommends screening for PAD in patients with diabetes1 A screening ABI should be performed in patients with diabetes • Those <50 years of age who have other risk factors associated with PAD • Smoking • Hypertension • Hyperlipidemia • Duration of diabetes • >10 years • Those >50 years of age • If normal an exercise • test should be • carried out • The ABI test • should be repeated • every 5 years • Foot care is also important in diabetic patients as PAD is a major contributor to diabetic foot problems2 1. American Diabetes Association. Diabetes Care 2003; 26: 3333–3341. 2. Estes JM, Pomposelli FB Jr. Diabet Med 1996: 13: S43–S57.
Patients with PAD are at risk of MI, ISand death CAPRIE data Cerebrovascularoutcome Coronaryoutcome 6 5.2 5.1 5 4.2 3.6 4 Clopidogrel 3 3-year cumulative event rate (%) Aspirin 2 1 0 Patients qualifying for CAPRIE on the basis of PAD Dormandy JA, Creager MA. Cerebrovasc Dis 1999;9(Suppl 1):1–128 (Abstr 4).
American Diabetes Association Consensus Statement 2003: PAD in people with diabetes • “It is recommended that patients with diabetes who are >50 years of age have an ABI performed. An ABI is also useful in patients with other PAD risk factors and in those with symptoms.”1 • “Patients with diabetes and PAD may benefit more by taking clopidogrel [than ASA].”1 1. American Diabetes Association. Diabetes Care: Vol 26: 12, Dec 2003
The Call to Action Paper highlighted 5 key action items Increase awareness of PAD and its consequences Improve treatment rates among patients who have been diagnosed with symptomatic PAD Call to action Paper Improve the identification of patients with symptomatic PAD 60% Increase the rates of early detection among the asymptomatic population Initiate a screening protocol for patients at high risk for PAD Belch JJF et al. Arch Intern Med 2003; 163: 884-892.