Download
1 / 28
290 likes | 600 Views
Mechanics Of Breathing. Lecture-2 Dr. Zahoor Ali Shaikh. Mechanics Of Breathing. Inspiratory Muscles 1. Diaphragm [major muscle contributes 75%] 2. External Intercostals contribute 25% Diaphragm

E N D
Mechanics Of Breathing Lecture-2 Dr. Zahoor Ali Shaikh
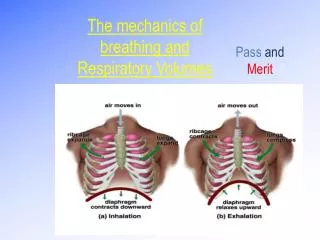
Mechanics Of Breathing • Inspiratory Muscles 1. Diaphragm [major muscle contributes 75%] 2. External Intercostals contribute 25% • Diaphragm • When Diaphragm contracts [on stimulation of phrenic nerve C3, C4, C5], it descends down and increases vertical diameter of the chest . • During quiet breathing, Diaphragm descends about 1cm but during deep inspiration it may descend up to 10cm.
Inspiratory Muscles 2.External Intercostals • Contraction of these muscles, whose fibers run downward and forward between the adjacent ribs, enlarge the thoracic cavity in lateral [side to side] and anterio-posterior [front to back] dimensions. • When external intercostal muscle contracts, they elevate the ribs and the sternum upward and outward. • Intercostal nerves activate these intercostal muscles.
Inspiration • Before Inspiration, intra-alveolar pressure is equal to atmospheric pressure (760mmHg) so no air is flowing into or out of lungs. • As the thoracic cavity enlarges [due to contraction Inspiratory muscles] the lungs also expand to fill the large thoracic cavity. • As the lungs enlarge, the intra-alveolar pressure drops by 1mmHg to 759mmHg, therefore, air flows inside, down the pressure gradient from higher atmospheric pressure to lower pressure.
Inspiration • Air enters the lungs till pressure equalizes [atmospheric and alveolar]. Note : Air flows into the lungs because of fall in the intra-alveolar pressure brought about by lung expansion due to enlargement of thoracic cavity due to contraction of inspiratory muscles.
Intra-pleural Pressure during Inspiration • During Inspiration, the intra-pleural pressure falls to 754mmHg [-6mmHg], as a result of expansion of the thorax. • Please note – Intra-pleural pressure before inspiration is 756mmHg [-4mmHg].
Accessory Muscles Of Inspiration • Forceful or deep inspiration can be brought about by contraction of accessory muscles of inspiration. They work with diaphragm and external-intercostal. Accessory Inspiratory Muscles Are: - Sternocleidomastoid - Scalenus - Trapizus - Pectoralis major
Accessory Muscles Of Inspiration • Contraction of Accessory muscles causes lifting of sternum and elevation of first two ribs, enlarging the upper portion of thoracic cavity. • As the thoracic cavity increases even further, lungs expand more, dropping intra-alveolar pressure further. • Therefore, more inward flow of air occurs.
Expiration • Expiration is passive process. • It occurs due to the relaxation of Inspiratory muscles i.e. diaphragm and external-intercostal muscle. • As diaphragm and external-intercostal muscle relax, the chest wall and stretched lungs recoil to their original [pre-Inspiratory] size, due to their elastic properties. • As the lungs recoil and become smaller in size, the intra-alveolar pressure rises by 1mmHg [761mmHg].
Expiration • As intra-alveolar pressure increases, air leaves the lungs down its pressure gradient from high intra-alveolar pressure to lower atmospheric pressure. • Air flow stops when intra-alveolar pressure becomes equal to atmospheric pressure.
Muscles of Forced Expiration • Muscles of forced [active] expiration are: - Internal-intercostal muscles - Abdominal muscles [rectus abdominas, transverse -abdominas ,external oblique, internal oblique] • NOTE • During quiet breathing, expiration is passive process. It occurs due to relaxing of inspiratory muscles. • Forceful expiration which is active process, we need contraction of forced expiratory muscles.
Muscles of Forced Expiration • Contraction of abdominal muscles decrease the vertical diameter of thorax. • Contraction of internal-intercostal muscles pull the ribs downward and inward, flattening the chest wall and decreasing the size of thoracic cavity [this action is opposite of external-intercostal muscles which pull the chest upward and outward].
Muscles of Forced Expiration • Contraction of expiratory muscles decreases the volume of thoracic cavity, lung volume decreases, intra-alveolar pressure increases, therefore, air leave the lung. • Lungs are emptied more during forceful expiration [during active expiration as compared to passive expiration].
Summary of Inspiration & Expiration • Normal Inspiration is active process due to contraction of diaphragm and external-intercostal muscles. • Normal Expiration is passive process due to relaxation of diaphragm and external-intercostal muscles. • Forceful inspiration - we use accessory muscles of inspiration e.g. sternomastoid, sclene etc. • Forceful expiration – we use accessory muscles of expiration e.g. internal-intercostal and abdominal muscles.
Clinical Application • Inspiratory muscles • Diaphragm which contributes to 75%, if paralyzed due to nerve damage or muscle disorder, it leads to severe respiratory impairment. • External-intercostal which contribute to 25%, if paralyzed, it does not seriously affect the breathing.
Air way resistance affects Air flow • Air flow depends on the resistance offered by air ways (bronchi and bronchioles). • Resistance will increase if the radius of conducting air ways (bronchi) gets smaller. • Air ways are supplied by Autonomic Nervous System [ANS]. • Parasympathetic ANS – causes broncho-constriction (decreases the radius of bronchioles) therefore increases the air way resistance. • Sympathetic ANS and Epinephrine They cause broncho-dilation (increase the radius of bronchioles) therefore decrease the air way resistance.
Air way resistance • Nowadays new drugs e.g. ventolin which act on β2 receptors which are present in bronchi (air ways) cause broncho-dilation. • They are commonly used for Bronchial Asthma.
Clinical Application • Chronic Obstructive Pulmonary Disease [COPD] • In COPD, there is increased air way resistance due to narrowing of lumen of lower air ways. • Patient with COPD have difficulty in breathing. • COPD applies to 3 diseases: 1. Chronic-Bronchitis 2. Bronchial Asthma 3. Emphysema
Chronic-Bronchitis • Affects lower respiratory airways. • It is triggered and ppt by cigarette smoking, polluted air and allergens. • Due to chronic irritation – air way is narrowed due to thickening of its lining, cilia lining the airways are also affected, therefore, mucus can not be removed satisfactorily. • Pulmonary Bacterial Infection are common.
Bronchial Asthma • Air way obstruction occurs due to - thickening of airway walls due to inflammation. - increased secretion of mucus. - airway constriction [spasm of smooth muscle in walls of airways] due to exposure to dust, pollen, cigarette smoking, infection, severe exercise. - increased airway resistance causes more difficulty during expiration than inspiration, causing wheeze.
Emphysema • Emphysema is characterized by - collapse of small airways - breakdown of alveolar walls - increased airway resistance • Emphysema is irreversible condition. • Emphysema can occur due to chronic exposure to irritants e.g. cigarette smoking due to release of enzyme trypsin released from alveolar macrophages. • This enzyme trypsin causes destruction of lung tissue.
What You Should Know From This Lecture • Muscles of Inspiration [Diaphragm and External-intercostal] and their function. • Muscles of Forced Inspiration [Accessory Muscles]. • Normal Expiration is passive process. • Muscles of Forced Expiration [Accessory Muscles] • Atmospheric Pressure, Intra-Alveolar Pressure, Intra-Pleural Pressure. • Airway Resistance. • Effect of Parasympathetic ANS and sympathetic ANS on airways [bronchi and bronchioles]. • Effect of ventolin on airways. • Chronic Obstructive Pulmonary [Lung] Diseases. - Chronic-Bronchitis, Bronchial Asthma, Emphysema.