Download
1 / 56
601 likes | 912 Views
Agents Affecting Mineral Ion Homeostasis and Bone Turnover. Agents Affecting Mineral Ion Homeostasis and Bone Turnover. Understanding some basic physiology and Pathophysiology Mineral Ion homeostasis Endocrinology of Ca 2+ & Phosphate metabolism pharmacotherapeutic options.

E N D
Agents Affecting Mineral Ion Homeostasis and Bone Turnover • Understanding some basic physiology and Pathophysiology • Mineral Ion homeostasis • Endocrinology of Ca2+ & Phosphate metabolism • pharmacotherapeutic options
Physiology of Mineral Ion Homeostasis • Calcium • ionized Ca2+, is an important component of current flow across excitable membranes (muscle contraction, fusion, and release of storage vesicles) • as a second messenger (intracellular < µM) • blood coagulation and support the formation and continuous remodeling of the skeleton (extracellular mM).
Calcium • The body content of calcium in healthy adult men and women, respectively, is ~1300 and 1000 g, of which >99% is in bone and teeth. • Although the portion of calcium in extracellular fluids is small, this fraction is stringently regulated within narrow limits.
Calcium • In adult humans, the normal serum calcium concentration ranges from 8.5-10.4 mg/dL (4.25-5.2 mEq/L, 2.1-2.6 mM) and includes three distinct chemical forms of Ca2+: ionized (50%), protein-bound (40%), and complexed (10%). • The concentration of ionized Ca2+ in human plasma is ~1.2 mM.
Calcium • Only diffusible calcium (i.e., ionized plus complexed) can cross cell membranes. • Albumin accounts for some 90% of the serum calcium bound. • Smaller percentages are bound to β-globulin, α2-globulin, α1-globulin, and γ-globulin. • The remaining 10% of the serum calcium is complexed in ion pairs with small polyvalent anions (phosphate and citrate).
Calcium • Ionized Ca2+ is the physiologically relevant component, mediates calcium's biological effects, and, when perturbed, produces the characteristic signs and symptoms of hypo- or hypercalcemia. • The extracellular Ca2+ concentration is tightly controlled by hormones that affect calcium entry at the intestine and its exit at the kidney; when needed, these same hormones regulate withdrawal from the large skeletal reservoir.
Calcium Stores • The skeleton contains 99% of total body calcium in a crystalline form resembling the mineral hydroxyapatite in bone reflects the net effect of bone resorption and bone formation, coupled with aspect of bone remodeling. • Tahe steady-state content of calcium. • labile pool of bone Ca2+ exchanges readily with interstitial fluid. • This exchange is modulated by hormones, vitamins, drugs, and other factors that directly alter bone turnover or that influence the Ca2+ level in interstitial fluid.
Calcium Absorption and Excretion • Milk and dairy products (~75%). • The adequate intake value for calcium is 1300 mg/day in adolescents and 1000 mg/day in adults. • After age 50, the adequate intake is 1200 mg/day. • Median intakes of calcium for boys and girls 9 years of age of 865 and 625 mg, respectively, and a median daily calcium intake of 517 mg for women >50 years of age.
Calcium absorption and excretion • The efficiency of intestinal Ca2+ absorption is inversely related to calcium intake (activation of Vit. D). • Steatorrhea, diarrhea, or chronic malabsorption promote fecal loss of Ca2+ • Drugs such as glucocorticoids and phenytoin, depress intestinal Ca2+ transport (PTH, frusemide and thiazides).
Phosphate • Phosphate is an essential component of all body tissues, present in plasma, extracellular fluid, cell membrane phospholipids, intracellular fluid, collagen, and bone tissue. • More than 80% of total body phosphorus is found in bone, and ~15% is in soft tissue. • Additionally, phosphate subserves roles as a dynamic constituent of intermediary and energy metabolism and as a key regulator of enzyme activity.
Phosphate • Biologically, phosphorus (P) exists in both organic and inorganic (Pi) forms. Organic forms include phospholipids and various organic esters. • In extracellular fluid, the bulk of phosphorus is present as inorganic phosphate in the form of NaH2PO4 and Na2HPO4; at pH 7.4, the ratio of disodium to monosodium phosphate is 4:1, so plasma phosphate has an intermediate valence of 1.8.
Phosphate • Owing to its relatively low concentration in extracellular fluid, phosphate contributes little to buffering capacity. • The aggregate level of inorganic phosphate (Pi) modifies tissue concentrations of Ca2+ and plays a major role in renal H+ excretion. • Within bone, phosphate is complexed with calcium as hydroxyapatites having the general formula Ca10(PO4)6(OH)2 and as calcium phosphate.
Absorption, Distribution, and Excretion • Phosphate is absorbed from and, to a limited extent, secreted into the GI tract. • Transport of phosphate from the intestinal lumen is regulated by vitamin D. • Renal phosphate absorption is regulated by a variety of hormones and other factors; the most important is PTH.
Hormonal Regulation of Calcium and Phosphate Homeostasis • A number of hormones interact to regulate extracellular calcium and phosphate balance. The most important are parathyroid hormone (PTH) and 1,25-dihydroxyvitamin D (calcitriol), which regulate mineral homeostasis by effects on the kidney, intestine, and bone.
Parathyroid Hormone • PTH is a polypeptide hormone that helps to regulate plasma Ca2+ by affecting bone resorption/formation, renal Ca2+ excretion/reabsorption, and calcitriol synthesis (thus GI Ca2+ absorption). • Chemistry • single polypeptide chains of 84 amino acids. • residues 1–27 are required for optimal binding to the PTH receptor and hormone activity.
PTH Synthesis, Secretion, and Immunoassay • PTH is synthesized as a 115-amino-acid translation product called preproparathyroid hormone. • PTH(7–84) accumulate significantly during renal failure . • competing with PTH(1–84). • PTH(1–84) has a t1/2 in plasma of ~4 minutes; removal by the liver and kidney accounts for ~90% of its clearance.
Physiological Functions of PTH • The primary function of PTH is to maintain a constant concentration of Ca2+ and Pi in the extracellular fluid. • The principal processes regulated are renal Ca2+ and Pi absorption, and mobilization of bone Ca2+. • PTH also affects a variety of tissues not involved mineral ions homeostasis (cartilage, VSM, placenta, liver, panceratic islets, brain, dermal fibroblasts, and lymphocytes). • PTH receptors (PTH1R or PTH/PTHrP); PTH2 receptor; CPTH.
Regulation OF Secretion of PTH • Plasma Ca2+ is the major factor regulating PTH secretion. • As the concentration of Ca2+ diminishes, PTH secretion increases. • Sustained hypocalcemia induces parathyroid hypertrophy and hyperplasia. • Conversely, if the concentration of Ca2+ is high, PTH secretion decreases. • Ca2+ itself appears to regulate parathyroid gland growth as well as hormone synthesis and secretion.
PTH Secretion • Changes in plasma Ca2+ regulate PTH secretion by the plasma membrane–associated calcium-sensing receptor (CaSR) on parathyroid cells. • Reduced occupancy of CaSR by Ca2+ has apposite effect, thereby promotion PTH secretion . • Calcitrioldirectly suppresses PTH gene expression.
PTH Effects on Bone & kidney • PTH exerts both catabolic and anabolic effects on bone. • Chronically elevated PTH enhances bone resorption and thereby increases Ca2+ delivery to the extracellular fluid, whereas intermittent exposure to PTH promotes anabolic actions. • PTH Effects on Kidney- Ca2+, phosphate, other ions, and calcitriol synthesis.
Integrated Regulation of Extracellular Calcium Concentration by PTH
Vitamin D • Vitamin D is actually a hormone rather than a vitamin; it is synthesized in mammals and, under ideal conditions, probably is not required in the diet. • Receptors for the activated form of vitamin D are expressed in many cells that are not involved in calcium homeostasis, including hematopoietic cells, lymphocytes, epidermal cells, hair follicles, adipose tissue, pancreatic islets, muscle, and neurons.
Physiological Functions and Mechanism of Action • Calcitriol augments absorption and retention of Ca2+ and phosphate. • Calcitriol acts to maintain normal concentrations of Ca2+ and phosphate in plasma by facilitating their absorption in the small intestine, by interacting with PTH to enhance their mobilization from bone, and by decreasing their renal excretion. It also exerts direct physiological and pharmacological effects on bone mineralization. • The mechanism of action of calcitriol is mediated by its interaction with VDR. • TRPV6 Ca2+ channels, calbindin.
Intestinal Absorption of Calcium • Calcium is absorbed predominantly in the duodenum. • Calcitriol increases the transcellular movement of Ca2+ from the mucosal to the serosal surface of the duodenum. • TRPV6 mediates calcium entry and is vitamin D dependent.
Transcellular Ca2+ transport in the intestine (duodenum/jejunum). Ca2+ enters the cells via TRPV6 channels, and Ca2+-binding proteins such as calbindin D9K facilitate Ca2+ transport to the basolateral membrane. Ca2+ can then be extruded by mechanisms that include the NCX1 Na+/Ca2+ exchanger and/or the Ca2+ATPase termed PMCA1b. VitD may upregulate the expression of both TRPV6 and PMCA1b. B: Pi transport in the intestine (primarily in jejunum). Some passive paracellular Pi transport may occur, although a transcellular mechanism is likely the primary means of Pi transport. Pi enters the cell via the luminal Na+/Picotransporter, NPT2b, and leaves the cell by an as yet undiscovered mechanism. VitD may stimulate NPT2b transcription and/or affect transporter activity.
Other Effects of Calcitriol • maturation and differentiation of mononuclear cells and influencing cytokine production and immune function. • cancer therapy • Psoriasis treatment • function of skeletal muscle, brain, and blood pressure
Calcitonin • Calcitonin is a hypocalcemic hormone whose actions generally oppose those of PTH. • Calcitonin is a 32-amino-acid peptide. • The thyroid parafollicular C cells are the site of production and secretion of calcitonin. • Calcitonin is the most potent peptide inhibitor of osteoclast-mediated bone resorption and helps to protect the skeleton during periods of "calcium stress" , such as growth, pregnancy, and lactation.
Regulation of Secretion • The biosynthesis and secretion of calcitonin are regulated by the plasma Ca2+ concentration. • Calcitonin secretion increases when plasma Ca2+ is high and decreases when plasma Ca2+ is low.
Mechanism of Action • calcitonin receptors • The hypocalcemic and hypophosphatemic effects of calcitonin are caused predominantly by direct inhibition of osteoclastic bone resorption. • Calcitonin interacts directly with receptors on osteoclasts to produce a rapid and profound decrease in ruffled border surface area, thereby diminishing resorptive activity. • Plasma phosphate concentrations are lowered owing also to increased urinary phosphate excretion.
Fibroblast Growth Factor 23 and Klotho • FGF23 is a hypophosphatemic hormone whose actions generally parallel those of PTH but with effects restricted to regulation of renal Pi absorption and vitamin D biosynthesis. • Klotho is a membrane protein that serves as an essential cofactor in the transduction of FGF23 signaling. • FGF23 is secreted in response to dietary phosphorus load, and its main function is the promotion of urinary phosphate excretion and the suppression of active vitamin D production by the kidney.
Bone Physiology • The skeleton is the primary structural support for the body and also provides a protected environment for hematopoiesis. • Skeletal Organization • Appendicularor peripheral • axial, or central • Bone Remodeling
Disorders of Mineral Homeostasis and Bone • Abnormal Calcium Metabolism • Hypercalcemia • fatigue, muscle weakness, anorexia, depression, diffuse abdominal pain, and constipation. • Newly diagnosed hypercalcemia in hospitalized patients is caused most often by a systemic malignancy, either with or without bony metastasis. • Hypocalcemia • Tetany, paresthesias, increased neuromuscular excitability, laryngospasm, muscle cramps, and tonic-clonic convulsions.
Disturbed Phosphate Metabolism • Dietary inadequacy very rarely causes phosphate depletion. • Hyperphosphatemia is an important component of the bone disease seen in chronic renal failure. • The increased phosphate level reduces the serum Ca2+ concentration, which, in turn, activates the parathyroid gland calcium-sensing receptor, stimulates PTH secretion, and exacerbates the hyperphosphatemia.
Disorders of Vitamin D • Hypervitaminosis D • derangements in calcium metabolism (hypercalcemia) • Digoxin toxicity • congenital supravalvular aortic stenosis • Vitamin D Deficiency • Inadequate absorption of Ca2+ and phosphate • Children (rickets) • Adults (osteomalacia)
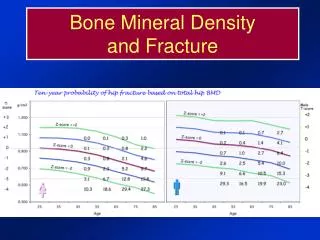
Osteoporosis • Osteoporosis is a condition of low bone mass and microarchitectural disruption that results in fractures with minimal trauma. • Osteoporosis is the result of multiple physical, hormonal, and nutritional factors acting alone or in concert.
Pharmacological Treatment of Disorders of Mineral Ion Homeostasis and Bone Metabolism • Hypercalcemia • fluid resuscitation • loop diuretics • Corticosteroides • Calcitonin • Intravenous Biophosphonates (pamidronate, zoledronate) • Hypocalcemia • Calcium chloride, Calcium gluconate (IV) • Calcium carbonate (oral)
Therapeutic Indications oF Vitamin D The major therapeutic uses of vitamin D may be divided into four categories: • prophylaxis and cure of nutritional rickets. • treatment of metabolic rickets and osteomalacia, particularly in the setting of chronic renal failure. • treatment of hypoparathyroidism. • prevention and treatment of osteoporosis.
Calcitonin • Diagnostic Uses of Calcitonin • Calcitonin is a sensitive and specific marker for the presence of medullary thyroid carcinoma (MTC), a neuroendocrine malignancy originating in thyroid parafollicular C cells. • Therapeutic Uses • Calcitonin lowers plasma calcium and phosphate concentrations in patients with hypercalemia; this effect results from decreased bone resorption and is greater in patients in whom bone turnover rates are high. • Hypercalcemia
Bisphosphonates • They are used extensively in conditions characterized by osteoclast-mediated bone resorption, including osteoporosis, steroid-induced osteoporosis, Paget's disease, tumor-associated osteolysis, breast and prostate cancer, and hypercalcemia. • Calcium supplements, antacids, food or medications containing divalent cations, such as iron, may interfere with intestinal absorption of bisphosphonates. • Recent evidence suggests that second- and third-generation bisphosphonates also may be effective anticancer drugs.