Download
1 / 25
250 likes | 444 Views
LACERATIONS OF THE LEG AND FOOT. BY S. SUPALERK. Introduction. Any injury to the lower extremity (especially the foot ) jeopardizes the ability to walk From simple plantar puncture wounds to catastrophic lawn mower injuries

E N D
LACERATIONS OF THE LEG AND FOOT BY S. SUPALERK
Introduction • Any injury to the lower extremity (especially the foot ) jeopardizes the ability to walk • From simple plantar puncture wounds to catastrophic lawn mower injuries • Soil contamination , risk of infection , worsening scarring , slowing healing
Clinical features • History • Time interval : increase incidence of infection • Mechanism of injury : underling tissue • Risk of retained foreign body • Degree of potential contamination • Complaint any new paresthesia , anesthesia weakness or loss of function suggests a nerve vascular or tendon injury prompting a careful examination
Past medical history • Tetanus immunization status • Condition increase risk for infection or delayed wound healing ( DM , immunosuppression ) and risk of bacteremia ( valvular heart disease , asplenia ) • Other medication
Physical examination • Location • Length • Depth • Shape of wound • Weight bearing surface • Distal sensory nerve function • Motor function • Vascular integrity
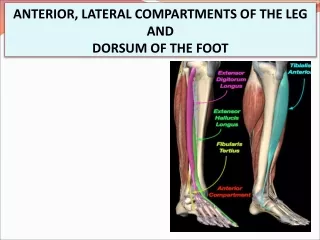
Nerve : light touch , static two-point discrimination • Superficial peroneal N. : foot eversion • Deep peroneal N. : foot inversion , ankle dorsiflexion • Posterior tibial N. : ankle plantar flexion • Tendon : direct visual because partially lacerated tendon can mimic normal fuction • Foreign bodies
CBC ESR CRP H/C Radiographic imaging Foreign body Fracture Joint space CT MRI Ancillary studies
Treatment Age considerations • Elderly • thin skin , decrease subcutaneous fat • Medical condition : delay wound healing • Tetanus immunization • Child • Difficulty limit movement • Contaminated wound • The smaller the child, the larger the dressing
Wound anesthesia • Sensory examination precede anesthesia • Dorsum foot , local anesthesia • Plantar surface , nerve blocks (sural , posterior tibial ) • Toes , digital nerve blocks • Topical anesthetic poorly effective on dense epidermis
Wound preparation and repair • Wound irrigation • anesthesia • Dry field exploration : tendon , FB • LW multiple layered closure decrease tension and simple interrupted , horizontal mattress suture use moderate tension , large LW avoid running sutures , infection • Debridement to remove devitalized tissue decrease risk of wound complication
Timing of closure , delay in closure • Delay primary closure less than 6 hr in case delayed presentation or contamination : pack saline soaked gauze • Antibiotic • reevaluated case
Plantar laceration • Pron position • Heavy , large suture needles and thick thread penetrate the hypertrophied epidermis and dermis of foot and sole , large curved cutting needle • Simple interrupted sutures • Tissue loss or under tension use vertical mattress suture • Avoid adhesive tapes , tissue adhesives , staples
Dorsal laceration • Nonabsorbable monofilament suture material • Running sutures are acceptable • Under select circumstances adhesive tapes with splints 5-7 days
Inter digital laceration • Between toe very difficult to repair • Simple interrupted suture • When the web involve neurovascular , the skin usually closed without any subsequent consideration to repair neurovascular
Skin laceration Wound over the anterior tibial surface are under considerable tension suggest multiple layered closure Elderly extremely thin and difficulty for closure suggest multiple layered Elastic bandage is placed over a generous dressing Weight bearing limited for 5 days Alternative : deep reinforced sutures placed through adhesive strips laid down parallel to the wound edges has been recently described
Knee laceration Joint capsule penetration , LW of patellar and quadriceps tendons should be assessed Common peroneal nerve is prone to injury check inversion , eversion , dorsiflexion Deep popliteal wound : popliteal artery ( minimal collateral circulation distal to knee ) , tibial nerve Mark active skin tension : knee immobilized
Tendon laceration Repair tendon laceration in foot depend on functional impairment Tendon at Mid foot and forefoot can go unrepaired ( without sacrificing any necessary foot function ) can close skin and splint Extensor hallucis longus or tibialis anterior : call orthopedist because dorsiflexion of the great toe and foot important in walking and running Achilles tendon is first palpated for defects : Thomson test
Repair a few days to weeks after initial injury Skin closure , splinting of the foot Antibiotic prophylaxis Non-weight bearing Follow up orthopredist
Tissue loss and Amputation • Major tissue loss as well as toe amputation • Tissue grafts and flap reconstruction by an orthopedist or plastic surgeon • Serve part : • wash gently with sterile saline • wrapped in saline-soak gauze • placed in plastic bag and closed • placed ice water bath
Retained foreign bodies Nonreactive FB ( glass ) is show chronic pain or chronic discomfort during walk if not removed Reactive organic material must aggressively sought and removed Fluoroscopy can use to help locate and remove radiopaque FB
Hair tourniquet Syndrome Strangulation and digital ischemia seen during infancy : long strand of hair wrapped around a toe
Disposition Bulky dressing is applied to plantar surface Weight-bearing is avoided for at least 5 days Elevation : decrease swelling and infection risk Typically removed sutures in 10 – 14 days
Prophylactic Antibiotic Use • Clinical adjustment according • Degree of contamination • Presence of foreign body • Presence of associated injury • Host factors
Amoxicillin - Clavulanate • Animal bite : staphylococcus , streptococcus , pasteurella • Asplenic or immunocompromised sustain dog bite : C.canimorsus. • Open fractures • S.aureus • First – generation cephalosporin • aminoglycoside
fluoroquinolone Compartment syndrome , myonecrosis , foot amputation • Freshwater stream • Aeromonas hydrophila • Gramnegative bacillus Aminoglycosides Trimethoprim – sulfamethoxazole fluoroquinolones