Download
1 / 37
420 likes | 1.2k Views
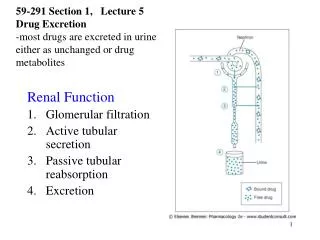
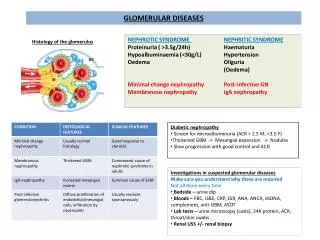
Tubular Processing of the Glomerular Filtrate. http://www.biologymad.com/resources/kidney.swf. Tubular Reabsorption is Selective and Quantitatively Large. Filtration = GFR X Plasma concentration Glomerular filtration and tubular reabsorption are very large

E N D
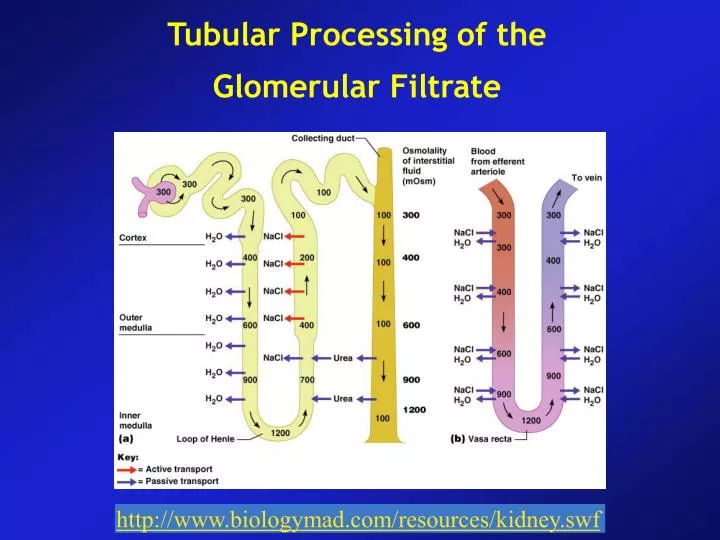
Tubular Processing of the Glomerular Filtrate http://www.biologymad.com/resources/kidney.swf
Tubular Reabsorption is Selective and Quantitatively Large • Filtration = GFR X Plasma concentration • Glomerular filtration and tubular reabsorption are very large • Glomerular filtration is non-selective, tubular reabsorption is highly selective • Some substances (glucose and aa) are almost completely reabsorbed • Certain waste products such as urea and creatinine are poorly reabsorbed
Tubular Reabsorption Includes Passive and Active Mechanisms • For a substance to be reabsorbed, it must first be transported • Across the tubular epithelial membranes into the renal interstitial fluid and then • Through the peritubular capillary membrane back into the blood flow • Peritubular capillaries behave much like the venous ends of most capillaries
Solutes can be transported through epithelial cells or between cells
Active Transport • Primary active transport • Secondary active transport • Co-transport • Counter transport • Pinocytosis • Active transport system for reabsorption of proteins
Transport maximum for substances that are actively reabsorbed • For most substances that are actively reabsorbed or secreted, there is a limit to the rate at which the solute can be transported (transport maximum)
Passive water reabsorption by osmosis is coupled mainly to sodium reabsorption
Reabsorption of chloride, urea and other solutes by passive diffusion • Passive diffusion of chloride through paracellular pathway • Urea is also passively reabsorbed from the tubule but to a much lesser extent • Almost none of the creatinine filtered is reabsorbed
Proxymal Tubular Reabsorption • Normally about 65% of the filtered load of Na and water are reabsorbed by the proxymal tubule • Proxymal tubule has a high capacity for active and passive reabsorption • Proxymal Tubule epithelial cells are highly metabolic
Secretion of organic acids and bases by the proxymal tubule • PT is also an important site for secretion of organic acids and bases e.g. bile salts, oxalate, urate and catecholamines • Excretion of harmful drugs and metabolites • Para-aminohippuric acid (PAH) is secreted so rapidly that average person can clear about 90% of the PAH from the plasma through the kidneys • Rate of PAH clearance can be used to estimate the renal plasma flow.
Solute and water transport in the Loop of Henle • Descending thin segment • Ascending thin segment • Ascending thick segment • Descending segment is highly permeable to water • Whereas the ascending segments are almost impermeable to water • The thick ascending segment has thick epithelial cells that have high metabolic rate and can reabsorb Na, Cl and K • Ca, Mg, HCO3 • Thin ascending segment has much lower absorption capacity
Solute and water transport in the Loop of Henle • Site of action for diuretics such as furosemid (inhibition of Na, 2 Cl and K co-transporter mechanism) • Paracellular reabsorption of Mg, Ca, Na and K in the thick henle • This segment has also a Na-H counter-transport mechanism • This segment is virtually impermeable to water
Distal Tubule • The very first portion of distal tubule (DT) forms part of the juxtaglomerular apparatus which provides feedback control of GFR and blood flow • About 5% of the filtered NaCl is reabsorbed in the early distal tubule • The thiazide diuretics (used for treatment of hypertension and heart failure) inhibit NaCl co-transport mechanism
Late Distal Tubule and Cortical Collecting Tubule • The second half of the distal tubule and proxymale collecting tubule have similar functional features • Principle cells and Intercalated cells • Principal cells reabsorb Na and secrete K (potassium) • These cells are therefore primary site of action for K-sparing diuretics such as triamterene • Aldosterone antagonists and receptor sites on principal cells • Intercalated cells secrete H and reabsorb HCO3 and K ions
Functional Characteristics of the late distal tubule and cortical collecting tubule
Functional Characteristics of the late distal tubule and cortical collecting tubule • The tubular membranes are almost completely impermeable to urea (it is passed to the collecting duct) • Both tubule segments reabsorb Na and its rate can be controlled by Aldosterone. At the same time these segments secrete K ions • Intercalated cells secrete H ions by an active hydrogene-ATPase mechanism • Permeability of these tubules to water is controlled by ADH
Medullary Collecting Duct (MCD) • Although MCD reabsorb less than 10% of the filtered water and Na, they are the final site for processing the urine and thus play an important role in the urine output of water and solutes • Permeability of MCD to water is controlled by ADH • Unlike the cortical collecting tubule, MCD is permeable to urea (formation of concentrated urine) • MCD is capable of secreting H ions against a high concentration gradient (playing a role in the regulation of acid-base balance)
Summary of Concentrations of Different Solutes in Different Tubular Segments
Tubular Fluid / Plasma Inulin concentration • Tubular fluid / plasma inulin level ratio can be used to measure water reabsorption by the renal tubules • This ratio is about 3.0 at the end of the proximal tubules • Inulin is not secreted or reabsorbed • A ratio of 3 means only one third of the water filtered remains in the tubule • 1/125 of the water filtered remains in the tubule (more than 99%)
TubuloGlomerular Balance • Intrinsic ability of the tubules to increase their absorption rate in response to increased tubular load (increased tubular inflow) • Tubuloglomerular feedback (first line of defense, GFR)
Peritubular Capillary and Renal Interstitial Fluid Forces • Hydrostatic and oncotic forces that govern the rate of reabsorption across the peritubular capillaries • Just as these physical forces that control filtration in the glomerular capillaries • Reabsorption of water and solutes from the renal tubules
Peritubular Capillary and Renal Interstitial Fluid Forces • Net reabsorptive force is about 10 mmHg, similar to that found in the glomerular capillaries but in the opposite direction
Effect of Arterial Pressure on Urinary Output • Pressure Diuresis • Pressure Natriuresis
Hormonal Control of Tubular Reabsorption • Precise regulation of body fluid volumes and solute concentrations requires the kidneys to excrete different solutes and water at variable rates, sometimes independently of one another.
Hormonal Control of Tubular Reabsorption • Aldosterone increases Na reabsorption and K secretion • Its primary site of action is on the principal cell of the proxymal collecting tubule • Angiotensin II increases Na and water reabsorption • Angiotensin II stimulates aldosteron secretion • It constricts the efferent arterioles • Angiotensin II directly stimulates Na reabsorption • ADH (Vasopressin) increases water reabsorption • ANP decreases Na and water reabsorption • Parathyroid hormone increases Ca reabsorption • Sympathetic activation increases Na reabsorption
Inulin Clearance can be used to estimate GFR • If a substance is freely filtered, not reabsorbed or secreted by the renal tubules, then its rate can be used to estimate the filtration rate • Inulin is not produced in the body, should be administered IV • Creatinine clearance and estimation of GFR • It is a by product of muscle metabolism
PAH clearance can be used to estimate Renal Plasma Flow • If a substance is completely cleared from the plasma, clearance rate of that substance is equal total renal plasma flow • PAH is about 90% cleared from the plasma • Filtration Fraction is Calculated from GFR / Renal Plasma Flow • GFR (inulin clearance) / renal plasma flow (PAH clearance)