Download
1 / 29
290 likes | 434 Views
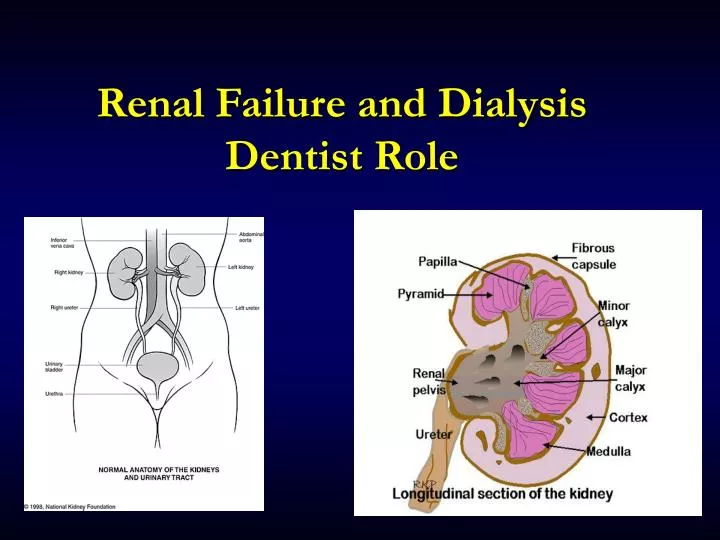
Renal Failure and Dialysis Dentist Role. What Are The Kidneys?. Nephrons are the functional units of the kidneys Within each kidney there are about 1 million nephrons Responsible for filtration & making urine Responsible for regulating electrolytes & acid/base balance

E N D
What Are The Kidneys? • Nephrons are the functional units of the kidneys • Within each kidney there are about 1 million nephrons • Responsible for filtration & making urine • Responsible for regulating electrolytes & acid/base balance • Responsible for converting Vit D to its active form Calcitriol • Responsible for removing wastes from the body • Erythropoietin Production : Formation of RBC • Normal renal function is monitored by GFR Normal GFR @125 ml/min • When GFR drops below 60ml/min, the patient will be symptomatic
Renal Laboratory Tests • Creatinine • With renal disease the kidney is not working properly, thus the serum creatinine will be high (it is not getting excreted) normal values 0.8 to 1.4 mg/dl • BUN: Blood Urea Nitrogen • With renal disease the kidney is not working properly, thus the BUN is higher than normal because the urea is not being excreted normal values 7 to 20 mg/dl • Creatinine Clearance: • Estimate of Glomerular Filtration Rate (GFR) Volume of Filtrate made by kidney/min • With renal disease the Creatinine Clearance will be low (kidney is not working well) • Normal Values: • Men 97-137 ml/min • Women 88-128 ml/min
What Happens When the Kidneys Aren’t Working Properly? • Build up of toxins within the body • Acid/Base imbalance • Vitamin D deficiency • Anaemia • Acute Renal Failure ESRD • Chronic Renal Failure ESRD
Acute Renal Failure • Definition: sudden loss of kidney function occurring over hoursdays • If untreated goes to Chronic Renal Failure or End Stage Renal Disease • Reversible if Aggressively treated • Etiology: • Prerenal • Intrarenal • Postrenal
Prerenal • The kidneys are not being perfused because: • Hypovolemic Shock (hemorrhage-internal or external) • Decreased cardiac output MI, CHF, Hypertension • Some interruption of blood flow to the kidneys
Intrarenal • The kidneys are damaged because: • Toxins • Glomerulonephritis • Stones • Infection-direct • Sepsis • Trauma • Clot • Obstruction
Postrenal • The outflow from the kidneys is blocked due to: • Urethral/Ureteral block • Infection • Urethral/Ureteral constricture
ARF: Treatment • Fix the Cause • Emergent Dialysis • Sodium Bicarb for Acid/Base imbalance • Lab Monitoring • Control of Potassium build-up • Maintenance of fluid balance: • Daily weights • Urine output measurements • Blood Pressure • Proper nutrition limit Na, K and Phosphorus
Chronic Renal Failure • Fairly uncommon • Insidious and progressive loss of kidney function is Irreversible • 2/3 – ¾ loss of function • Ends with End Stage Renal Disease
CRF: Causes • Diabetes Mellitus • Uncontrolled Hypertension • Glomerulonephritis • Neoplasia • Obstruction • Drugs Cocaine and Heroin • Amyloidosis • SLE • Polycystic Kidney Disease (Hereditary) • Age after the age of 40 you lose 1ml/min kidney kidney function/yr
CRF: Stages • Stage 1 • Persistent albuminuria (protein in urine suggesting improper renal filtration • Stage 2 • GFR 60-89 • Stage 3 • GFR 30-59 • Stage 4 • GFR 15-29 • Stage 5 • GFR <15 Also Known as End Stage Renal Disease
Weight loss (anorexia) Lethargy (anemia), Pitting Edema Chronic azotemia Nail abnormalities High Creatinine and BUN Seizures/ Tremors Coma Increased susceptibility to infection Dyspnea Confusion Weakness Altered Mental Status Decreased/No Urine Output Low EPO; shortened RBC life span Infertility Thrombocytopenia Bone Pain/ Fracture Among Many Others… CRF: Symptoms
CRF: Treatment • Treatment: • Treat Underlying chronic condition (DM, HTN, Infection, Neoplasm (benign or malignant)) • Antibiotics • Palliative and Supportive Therapy fluids and electrolytes • Vitamin B complex and anabolic steroids • Avoid nephrotoxic drugs • Hemo or peritoneal dialysis • Diet • Low protein cannot rid body of toxic metabolic products • Prognosis: poor long term
Sudden onset Reversible(usually) Temporary Oliguric or non-oliguric Oliguric - <400 cc/24 hr Non-oliguric - > 800cc/24 hr Insidious onset Progressive in its destruction of nephrons and renal structure Irreversible Acute vs. Chronic Renal Failure
End Stage Renal Disease • The endpoint of the progression of Acute or Chronic Renal Failure (if Acute did not resolve) • Can take 10-20 years to go from CRF to ESRD • Function of the kidney is <15% and usually <10%
ESRD: Causes • Same causes as Acute and Chronic Renal Failure: • Hypertension • Diabetes Mellitus • Long Term NSAID toxicity • Polycystic Kidney Disease • SLE • Glomerulonephritis • Congestive Heart Failure • …
ESRD: Death • Occurs from the build-up of toxic products within the body effecting each organ system
ESRD Treatment • Dialysis ( Haemo & Peritoneal ) • Dialysis basically acts as an external kidney • Usually 3 sessions/wk each session is 3-4 hours long • Patients always given heparin to prevent clotting of the AV access • Peritoneal Dialysis Is less efficient than hemodialysis • Kidney Transplant
Renal Transplant • Replacement of nonworking kidneys with donor kidney: one can survive with one functional kidney • Donor kidney is attached to renal artery and vein and ureter. Unless nonworking kidneys are infected, they are left in place
Oral Complications of Renal Disease • Anemia causes the oral mucosa to become more pale • Medications for renal disease cause xerostomia • Urea content causing metallic taste • Patients may have excessive bleeding • Hyperparathyroidism due to build up of phosphate and also due to Vitamin D not being activated allowing for Ca to be absorbed by the gut • Loss of Lamina Dura • Brown’s Tumor • Demineralization of Alveolar Bone
ESRD: Dental Considerations • Consult with Physician: • Make sure pt can be treated in outpatient setting • Pretreatment PT, PTT, Bleeding Time, INR, RFT, Hb • Monitor blood pressure in arm without shunt • Antibiotic prophylaxis • Drug selection may want to avoid NSAIDS
Dialysis: Dental Considerations • Indwelling Catheter is susceptible to infection Ab Prophylaxis • Try to avoid treatment dialysis days or at least 4 hours after dialysis due to possibility of bleeding • Best time to do dentistry on a patient undergoing dialysis: DAY AFTER
Transplant Patients: Dental Considerations • Pretransplant: • Get rid of all infection: • Extraction of: • Caries close to pulp • Periodontal Disease pockets > of = to 5mm • Unrestorable teeth • Aggressive Oral Hygiene • Postransplant: • 6 months post only emergent care • Remember pts will be pumped up with steroids to prevent graft rejection may want supplemental corticosteroids for stress
Antibiotic Prophylaxis or Dental Patients at Risk for Infection • “Vascular catheters, such as those required by patients undergoing dialysis, chemotherapy, or frequent administration of blood products, are susceptible to bacterial infections.” • Prophylax dialysis patients: • 2g Amoxicillin 1 hr prior to procedure • 600mg Clindomycin 1 hr prior toprocedure (if Pen allergy)