Download
1 / 33
350 likes | 452 Views
Is a Acute, Rapidly progressive & extensive necrosis of muscle accompained by gas formation & systemic toxicity due to contaminat ion of wound with pathogenic clostridia. O ccurs when bacteria invade healthy muscle from adjacent traumatized muscle or soft tissue

E N D
Is a Acute, Rapidly progressive &extensive necrosis of muscle accompained by gas formation & systemic toxicity due to contamination of wound with pathogenic clostridia. Occurs when bacteria invade healthymuscle from adjacent traumatized muscle or softtissue Malignant edema/anaerobic myositis/ clostridial myonecrosis Disease of war Civilian life-road accidents
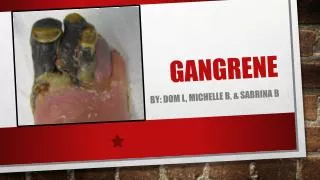
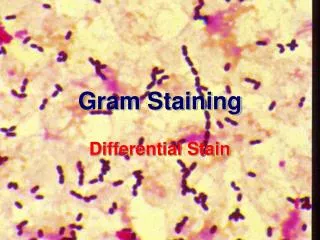
Gram staining of exudate from gas gangrene, Myonecrosis originated from infected umbilical stump
Predisposing factors An essential factor in the genesis of gas gangrene appears is trauma involvingdeep muscle. The trauma need not be severe but wound must be deep, necrotic, and without communicationto thesurface surgical incisions Compound fractures Diabetic ulcers Septic abortions Puncture wounds Gunshot wounds
Established pathogens - Cl.perfringens - cl.septicum Cl.novyi Less pathogenic- Cl.hitolyticum,Cl.fallux Doubt ful pathogens- Cl.bifermentans Cl.sporogens, Cl.sordelli cl.aerofoetidum,cl.tertium Facultative anaerobes- E coli, proteus, staphylococci
Clostridia have been isolated from the mucous membranes of humans, including the GI tract and the female genital tract. • Clostridia may also colonize the skin, especially around the perineum. • C perfringens produces 20 exotoxins. Alpha toxin - Lethal, necrotizing, hemolytic, cardiotoxic
1. Simple wound contamination- No invasion of underlying tissue, delay n wound healng 2.Anaerobic cellulitis- Clostridia invades fascial planes,nt muscle,minimal toxin prdn. 3.Anaerobic myositis- Invasion f healthy muscle tissue, Abundant toxin prodn.
Carbohydrates Fermentation Spores germinate Gas production In tissues Anaerobic environment PATHOGENESIS Incubation period is 1-7 days Distension of tissues Toxemia and death Interfering Blood supply Ischemia/ gangrene
Clostridia enter wound along with foreign particles / endogenous spread. Low oxygen tension - battle wound - ionised salt & silicic acid in soil- necrosis -Crushing tissue/tearing of arteries-anoxia -Extravasation of bld, Pr. In arteries Fall in redox potential,Eh & pH
Brk down of CHO & liberatn of aa-proliferation of anaerobes. Extravasated Hb & myoglobin are reduced. Anaerobic reduction of pyruvate to lactate -fall in Eh. Multiplication of clostridia & toxin production- lecithinase, alpha toxin collagenase,Hyaluronidase
Lecithinase- cell memb damage, cap. Permeability • Alpha toxin- impt cause of toxemia, lysis of erythrocytes • Collagenase-brk down tissues, liquefy musc. • Hyaluronidase-brk down inter cellular cement substances
Abundant production of gas Impairmnt of local bld supply & extnsion of areas of damage Profound toxemia,shock,hypotension, multple organ failure & death . Incubatn period- 7 hrs to 6 wks Cl.perfringens- 10-48 hrs Cl.septicum 2-3 days Cl.novyi 5-6 days
Crepitus Sponge-cake consistency Anxious frightened appearance in early stage Local pain Swelling of affected tissue Toxemia & shock- delerium & coma
Gram stain- Cl.perfringens-large no of regular,grm + bacilli with out spores Cl.septicum-Citron bodies & boat or leaf shaped pleomorphic bacilli. Cl.novyi-large bacilli with oval subterminal spores Cl.tetani/tetano morphum-slndr bacilli, terminal spore.
Films from the muscle-edges-affected area,tissue-necrotic area. Exudate-frm most active infection & depth of wound. Necrotic tissue & muscle fragment.
Gram staining of C. perfringens Clostridium perfringens on blood agar Flat, spreading colonies with hemolytic activity of the organism. A presumptive identification of C. perfringens can be made by detection of a zone of complete haemolysis (caused by the θ-toxin) and a wider zone of partial hemolysis (caused by the α-toxin), combined with the characteristic microscopic morphology.
Fresh/heated blood agar ( 5-6% agar )- + in Cl.perfringens,septicum Serum/egg yolk agar with Cl.perfringens anti toxin – Nagler rxn. Robertson cooked meat broth –heat resistant spores. Litmus milk–Cl.perfringens, stormy clot rxn
Surgery- impt prophylatic &therapeutic measure Uncompromised excision of affected part Hyper baric oxygen therapy Antibiotics -metronidazole iv before surgery & 8 hrly for 24 hrs -combination-metronidazole,gentamycin, amoxycillin .
Passive immunisation- Anti gas gangrene serum. Equine poly valent anti toxin Cl.perfringens-10,000 IU Cl.novyi – 10,000 IU Cl.septicum-5000 IU Uncertain efficacy & availability-rare
Positive Nagler Reaction Procedure of Nagler Reaction
Disfiguring or disabling permanent tissue damage Jaundice with liver damage Renal failure Sepsis Shock Coma Death
Management • The combination of aggressive surgical debridement and effective antibiotic therapy • penicillin G in dosages of 10-24 million u/d was the drug of choice. • Combination of penicillin and clindamycin combination of clindamycin and metronidazole is a good choice for patients allergic to penicillin.
Intensive care: Patients with gas gangrene frequently have end-organ failure and other concomitant serious medical conditions that require intensive supportive care. • Monitoring serum calcium • Adjuvant therapy: Recombinant human activated protein C
Hyperbaric oxygen (HBO) therapy Involves administration of 100% oxygen at 2.5-3 absolute atmospheres for 90-120 minutes 3 times a day for 48 hours, then twice a day as needed.
complication-Barotraumaticotitis, pneumothorax) and oxygen toxicity (myopia, seizures). • Other common adverse effects include claustrophobia.
Fasciotomy for compartment syndrome. • Irrigation should be performed with sterile normal saline solutions and3% liquid hydrogen peroxide. • Debridement • Perform daily debridement
wounds treated elsewhere and closed- reopen them, clean them, and leave them open with negative-pressure wound dressing therapy (if available) or just a sterile dressing. • Amputation of the extremity • Abdominal involvement requires excision of the body wall musculature. • Uterine gas gangrene following septic abortion usually necessitates hysterectomy.