Download
1 / 1
10 likes | 94 Views
#1113: Detection of circulating tumor cells from renal carcinoma patients: experiences of a two-center study Meye A 1 , Blümke K 2 , Bilkenroth U 1 , Schmidt U 1 , Füssel S 1 , Linne C 1 , Melchior AM 1,3 , Nippgen J 1 , Linne C 1 , Bartel F 2 , Heynemann H 3 , Taubert H 2 , and Wirth MP 1

E N D
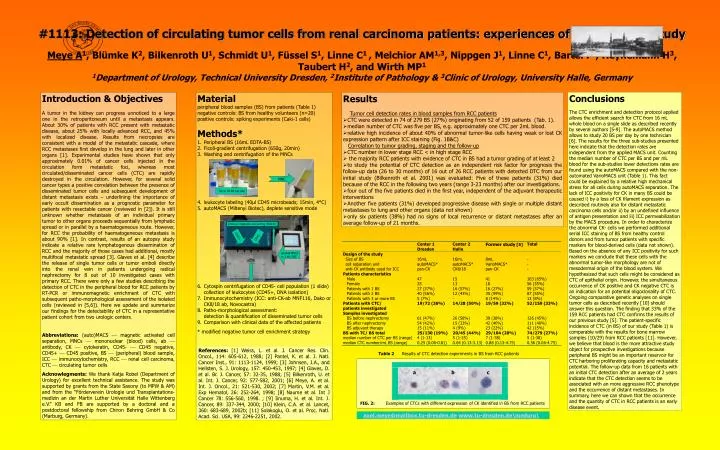
#1113: Detection of circulating tumor cells from renal carcinoma patients: experiences of a two-center study Meye A1, Blümke K2, Bilkenroth U1, Schmidt U1, Füssel S1, Linne C1 , Melchior AM1,3, Nippgen J1, Linne C1, Bartel F2, Heynemann H3, Taubert H2, and Wirth MP1 1Department of Urology, Technical University Dresden, 2Institute of Pathology & 3Clinic of Urology, University Halle, Germany Introduction & Objectives A tumor in the kidney can progress unnoticed to a large one in the retroperitoneum until a metastasis appears. About 30% of patients with RCC present with metastatic disease, about 25% with locally advanced RCC, and 45% with localized disease. Results from necropsies are consistent with a model of the metastatic cascade, where RCC metastases first develop in the lung and later in other organs [1]. Experimental studies have shown that only approximately 0.01% of cancer cells injected in the circulation form metastatic foci, whereas most circulated/disseminated cancer cells (CTC) are rapidly destroyed in the circulation. However, for several solid cancer types a positive correlation between the presence of disseminated tumor cells and subsequent development of distant metastasis exists – underlining the importance of early occult dissemination as a prognostic parameter for patients with resectable cancer (reviewed in [2]). It is still unknown whether metastasis of an individual primary tumor to other organs proceeds sequentially from lymphatic spread or in parallel by a haematogeneous route. However, for RCC the probability of haematogeneous metastasis is about 90% [1]. In contrast, results of an autopsy study indicate a relative rare lymphatogenous dissemination of RCC and the majority of those cases had additional, mostly multifocal metastatic spread [3]. Glaves et al. [4] describe the release of single tumor cells or tumor emboli directly into the renal vein in patients undergoing radical nephrectomy for 8 out of 10 investigated cases with primary RCC. There were only a few studies describing the detection of CTC in the peripheral blood for RCC patients by RT-PCR or immunomagnetic enrichment of CTC with subsequent patho-morphological assessment of the isolated cells (reviewed in [5,6]). Here we update and summarize our findings for the detectability of CTC in a representative patient cohort from two urologic centers. Abbreviations: (auto)MACS magnetic activated cell separation, MNCs mononuclear (blood) cells, ab antibody, CK cytokeratin, CD45- CD45 negative, CD45+ CD45 positive, BS (peripheral) blood sample, ICC immunocytochemistry, RCC renal cell carcinoma, CTC circulating tumor cells Acknowlegments: We thank Katja Robel (Department of Urology) for excellent technical assistance. The study was supported by grants from the State Saxony (to MPW & AM) and from the “Förderverein Urologie und Transplantations-medizin an der Martin Luther Universität Halle Wittenberg e.V.” KB and FB are supported by a doctoral and a postdoctoral fellowship from Chiron Behring GmbH & Co (Marburg, Germany). • Material • peripheral blood samples (BS) from patients (Table 1) • negative controls: BS from healthy volunteers (n=20) • positive controls: spiking experiments (Caki-1 cells) • Methods* • Peripheral BS (16mL EDTA-BS) • Ficoll-gradient centrifugation (650g, 20min) • Washing and centrifugation of the MNCs • leukocyte labeling (40µl CD45 microbeads; 15min, 4°C) • autoMACS (Miltenyi Biotec), deplete sensitive mode • Cytospin centrifugation of CD45- cell population (1 slide) collection of leukocytes (CD45+, DNA isolation) • Immunocytochemistry (ICC: anti-CK-ab MNF116, Dako or CK8/18 ab, Novocastra) • Patho-morphological assessment:detection & quantification of disseminated tumor cells • Comparison with clinical data of the affected patients • * modified negative tumor cell enrichment strategy Conclusions The CTC enrichment and detection protocol applied allows the efficient search for CTC from 16 mL whole blood on a single slide as described recently by several authors [5-9]. The autoMACS method allows to study 20 BS per day by one technician [6]. The results for the three sub-studies presented here indicate that the detection rates are independent from the applied MACS unit. Counting the median number of CTC per BS and per mL blood for the sub-studies lower detections rates are found using the autoMACS compared with the non-automated VarioMACS unit (Table 1). This fact could be explained by a relative high mechanical stress for all cells during autoMACS separation. The lack of ICC positivity for CK in many BS could be caused i) by a loss of CK filament expression as described routinely also for distant metastatic carcinoma cells and/or ii) by an undefined influence of antigen presentation and iii) ICC permeabilization by the MACS procedure. In order to characterize the abnormal CK- cells we performed additional serial ICC staining of BS from healthy control donors and from tumor patients with specific markers for blood-derived cells (data not shown). Based on the absence of any ICC positivity for such markers we conclude that these cells with the abnormal tumor-like morphology are not of mesodermal origin of the blood system. We hypothesized that such cells might be considered as CTC of epithelial origin. However, the simultaneous occurrence of CK positive and CK negative CTC is an indication for an potential oligoclonality of CTC. Ongoing comparative genetic analyses on single tumor cells as described recently [10] should answer this question. The finding that 33% of the 159 RCC patients had CTC confirms the results of our previous study [5]. The patient-specific incidence of CTC (in BS) of our study (Table 1) is comparable with the results for bone marrow samples (10/29) from RCC patients [11]. However, we believe that blood is the more attractive study object for prospective investigations because peripheral BS might be an important reservoir for CTC harboring proliferating capacity and metastatic potential. The follow-up data from 16 patients with an initial CTC detection after an average of 2 years indicate that the CTC detection seems to be associated with an more aggressive RCC phenotype and the occurrence of distant metastases. In summary, here we can shown that the occurrence and the quantity of CTC in RCC patients is an early disease event. • Results Tumor cell detection rates in blood samples from RCC patients • CTC were detected in 74 of 279 BS (27%) originating from 52 of 159 patients (Tab. 1). • median number of CTC was five per BS, e.g. approximately one CTC per 2mL blood. • relative high incidence of about 40% of abnormal tumor-like cells having weak or lost CK expression pattern after ICC staining (Fig. 1B&C) Correlation to tumor grading, staging and the follow-up • CTC number in lower stage RCC < in high stage RCC • the majority RCC patients with evidence of CTC in BS had a tumor grading of at least 2 • to study the potential of CTC detection as an independent risk factor for prognosis the follow-up data (26 to 30 months) of 16 out of 26 RCC patients with detected DTC from our initial study (Bilkenroth et al. 2001) was evaluated: Five of these patients (31%) died because of the RCC in the following two years (range 3-23 months) after our investigations. • four out of the five patients died in the first year, independent of the adjuvant therapeutic interventions • Another five patients (31%) developed progressive disease with single or multiple distant metastases to lung and other organs (data not shown) • only six patients (38%) had no signs of local recurrence or distant metastases after an average follow-up of 21 months. MNC Up to 20 BS per day immuno-magnetic cell sorting (MACS) CD45+ CD45- labeled MNCsin 1 mL PBS References: [1] Weiss, L. et al. J. Cancer Res. Clin. Oncol., 114: 605-612, 1988; [2] Pantel, K. et al. J. Natl. Cancer Inst., 91: 1113-1124, 1999; [3] Johnsen, J.A., and Hellsten, S. J. Urology, 157: 450-453, 1997; [4] Glaves, D. et al. Br. J. Cancer, 57: 32-35, 1988; [5] Bilkenroth, U. et al. Int. J. Cancer, 92: 577-582, 2001; [6] Meye, A. et al. Int. J. Oncol., 21: 521-530, 2002; [7] Martin, V.M. et al. Exp Hematol, 26: 252-264, 1998; [8] Naume et al. Int J Cancer 78: 556-560, 1998.; [9] Iinuma, H. et al. Int. J. Cancer, 89: 337-344, 2000; [10] Klein, C.A. et al. Lancet, 360: 683-689, 2002b; [11] Solakoglu, O. et al. Proc. Natl. Acad. Sci. USA, 99: 2246-2251, 2002. Table 2 Results of CTC detection experiments in BS from RCC patients a b c FIG. 2: Examples of CTCs with different expressionof CK identified in BS from RCC patients axel.meye@mailbox.tu-dresden.dewww.tu-dresden.de\meduro\