Download
1 / 21
220 likes | 649 Views
Meticulous Pathologic Evaluation to Ensure Negative Margins Facilitates a Low Risk of Local Recurrence of Dermatofibrosarcoma Protuburans (DFSP). Departments of Sarcoma and Cutaneous Oncology. Marilyn M. Bui, Jane L. Messina, Jeffrey M. Farma, Suroosh S. Marzban,

E N D
Meticulous Pathologic Evaluation to Ensure Negative Margins Facilitates a Low Risk of Local Recurrence of Dermatofibrosarcoma Protuburans (DFSP) Departments of Sarcoma and Cutaneous Oncology Marilyn M. Bui, Jane L. Messina, Jeffrey M. Farma, Suroosh S. Marzban, Vernon K. Sondak, Douglas Letson and Jonathan S. Zager
Introduction DFSP is a rare dermal tumor with limited metastatic potential but significant risk of local recurrence Controversy regarding margin width and the risk of local recurrence Debate also exists regarding the optimal method for margin evaluation We reviewed our DFSP experience to determine outcomes using 1-2 cm resection margins and total peripheral margin pathologic evaluation
Our Study IRB approved retrospective review of all DFSP patients treated with surgery at Moffitt Cancer Center between 1994 and 2008 Clinicopathological characteristics examined: Confirmation of diagnosis Margin width Number of excisions needed to achieve (-) margins Reconstruction techniques Postoperative radiation Local or distant recurrence
Standard Institutional Protocol Wide local excision with 1-2 cm margins Staged closure performed if unable to primarily close Meticulous pathologic analysis with en face sectioning for total peripheral margin analysis Re-excision of any positive margin Follow-up Every 6 months for 5 years by physical exam only If transformed DFSP include imaging of the thorax
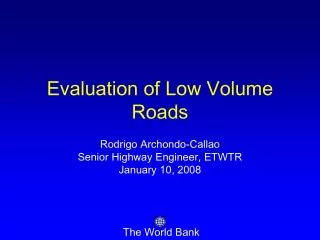
En Face Margin Technique 12 DFSP 3 9 6
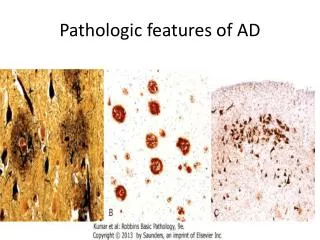
Pathologic Evaluation of Margins • DFSP resection specimens were submitted intraoperatively for gross examination • Additional tissue was taken when margin was positive • Frozen section was used judiciously • Tangential sections of the entire margin were submitted for histological examination after proper tissue fixation • CD34 immunostain used in difficult cases
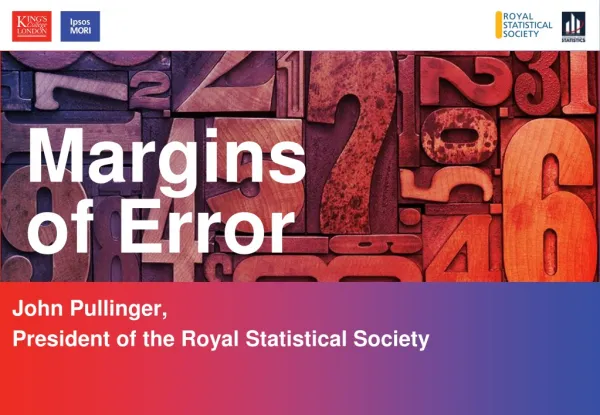
2 mm tangential sections removed from entire peripheral margin; Sections embedded with outer margin “face up” 12 3 12 12 9 DFSP 3 9 6 3 9 6 6 Pathologic Evaluation of Margins
When positive, additional 1 cm re-excisions were performed in the same fashion to achieve negative margin
Margins of Excision 35 Patients 27 (77%) had (–) margin after 1st excision 8 (33%) required multiple excisions 1 with a persistent (+) margin
Margins of Excision 6 Patients 4 (67%) had (-) margins after 1st excision 2 (33%) required multiple excisions
Margins of Excision 4 Patients 4 (100%) had (-) margins after 1st excision
Result: Margins of Excision • The median number of excision for negative margins was 1 (range 1-3) with 53% having a negative margin after 1 excision • The median excision margin was 1.5 cm (range 0.5-3) • 75% were closed primarily without skin grafts or flaps
Result: CD34 Immunostain • Used in 5 difficult cases • Proven useful where a sense dermal scar or small microscopic focus of DFSP
Result: Recurrence 35 Patients 27 (77%) had (–) margin after 1st excision 8 (23%) required multiple excisions 1 with a persistent (+) margin NO RECURRENCES 4 Patients 4 (100%) had (-) margins after 1st excision NO RECURRENCES 6 Patients 4 (67%) had (-) margins after 1st excision 2 (33%) required multiple excisions NO RECURRENCES 37 Patients 32 (86%) had (-) margin after 1st excision 5 (14%) required multiple excisions 1 with a persistent (+) margin 2 RECURRENCES
Result: Recurrence At a median follow-up of 44 months, 2 patients (2.4%) recurred locally Both in the head and neck region (2/13) Both with local recurrence underwent re-resection Time to recurrence was 13 months and 84 months
Conclusions Standard en face surgical excision in conjunction with meticulous pathologic evaluation of margins for all DFSP patients with repeat excision as necessary to achieve negative margins A very low recurrence rate (2.4%) was achieved with fairly narrow margins (medium 1.5 cm) This approach limits the number of patients who require wider resection margins, allowing primary closure in 75% of patients
Comments • It is misconception that WLE needs to be > 3 cm • A high local recurrence rate is most likely related to unrecognized persistence of tumor at the margins of resection • Experienced pathologists play a vital role in the successful multidisciplinary management of DFSP