Download
1 / 11
330 likes | 1.35k Views
Pneumothorax. Abdallah aljazzazi. Text. Defined as air in the pleural space leading to partial or complete collapse of the lung and occurs spontaneously or secondary to chest trauma. pneumothorax.

E N D
Pneumothorax Abdallah aljazzazi
Text Defined as air in the pleural space leading to partial or complete collapse of the lung and occurs spontaneously or secondary to chest trauma. pneumothorax
Spontaneous- SimpleWithout any underlying lung disease- ComplicatedOccurs as a complication of underlying lung disease Traumatic Types of Pneumothorax
Simple- Typically occurs in young men (typically tall and thin) and is the result of rupture of a pleural bleb which is thought to be due to a congenital defect in the connective tissue of the alveolar wall - Recurrence rate is 50% in 2 years- Spontaneous pneumothorax is commonest in young males, the male-to-female ratio being 6 : 1 Complicated- Most commonly secondary to COPD; other underlying conditions that might cause pneumothorax include asthma, interstitial lung disease (ILD), neoplasms, CF, and TB- More life-threatening because of lack of pulmonary reserve in these patients Spontaneous pneumothorax
Symptoms- Ipsilateral chest pain, usually sudden in onset - Dyspnea- Cough Physical signs- Decreased breath sounds over the affected side- Hyperresonance over the chest- Decreased or absent tactile fremitus on affected side- Mediastinal shift toward side of pneumothorax Clinical features
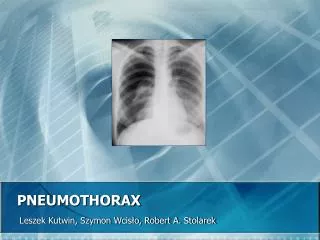
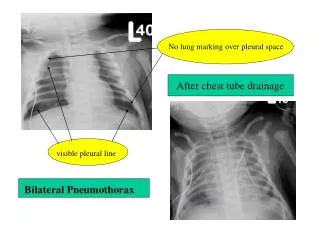
Imaging • CXR confirms the diagnosis- Shows the visceral pleural line - Loss of pulmonary markings over the left lung - Mediastinum is shifted away from the pneumothorax and diaphragm on the same side is pushed downwards with large pneumothoraces. • The size of a pneumothorax is estimated by measuring the distance from the lateral edge of the lung to the inner wall of the ribs. A distance >2 cm implies that the pneumothorax is at least 50%, and hence large in size. Left pneumothorax
If secondary : • Patients remain in hospital • Attempt aspiration only in minimally breathless patients,<50 years old with small pneumothoraces • Chest drain insertion indicated in all other patients • Oxygen given via a fixed-performance mask to patients with COPD Treatment **** Indications for surgical referral in patients with pneumothorax include persistent air leaks, recurrent pneumothorax and after a first pneumothorax in professions at risk (pilots, divers). All patients admitted to hospital should receive high-flow oxygen (10 L/min) to increase absorption of air from the pleural cavity.
Accumulation of air within the pleural space such that tissues surrounding the opening into the pleural cavity act as valves, allowing air to enter but not to escape. The accumulation of air under (positive) pressure in the pleural space collapses the ipsilateral lung and shifts the mediastinum away from the side of the pneumothorax. Most commonly iatrogenic following CPR or mechanical ventilation, can also follow trauma tension pneumothorax
Respiratory distress (If awake) Hypotension—cardiac filling is impaired due to compression of the great veins Distended neck veins Shift of trachea awayfrom side of pneumothorax on CXR Decreased breath sounds on affected side Hyperresonance to percussion on side of pneumothorax Jugular venous distention may be absent in a hypovolemic patient. Tracheal deviation is a late finding and often is not apparent on clinical examination. Practically, three findings are sufficient to make the diagnosis of tension pneumothorax: respiratory distress or hypotension, decreased lung sounds, and hypertympany to percussion. Chest x-ray findings that may be visualized include deviation of mediastinal structures, depression of the hemidiaphragm, and hypo-opacification with absent lung markings. Do not obtain CXR if a tension pneumothorax is suspected. Immediately decompress the pleural space via large-bore needle or chest tube Clinical features
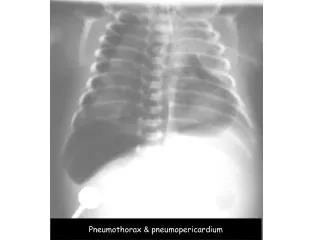
Xray findings • Contralateral mediastinal displacement • Collapse ipsilateral lung • Flattening or inversion ipsilateral diaphragm • Widening ipsilateral intercostal spaces • Flattening ipsilateral heart border • Hyperlucent ipsilateral thorax
Must be treated as a medical emergency If the tension in the pleural space is not relieved, the patient is likely to die of hemodynamic compromise(inadequate CO or hypoxemia). Immediately perform chest decompression with a large-bore needle in the second or third intercostal space in the midclavicular line, followed by chest tube placement. Treatment