Download
1 / 173
1.73k likes | 1.91k Views
Hemodynamic Disorders Thromboembolic Disease Shock. Overview. Edema (increased fluid in the ECF) Hyperemia (INCREASED flow) Congestion (INCREASED backup) Hemorrhage (extravasation) Hemostasis (keeping blood as a fluid) Thrombosis (clotting blood) Embolism (downstream travel of a clot)

E N D
Hemodynamic Disorders • Thromboembolic Disease • Shock
Overview • Edema (increased fluid in the ECF) • Hyperemia (INCREASED flow) • Congestion (INCREASED backup) • Hemorrhage (extravasation) • Hemostasis (keeping blood as a fluid) • Thrombosis (clotting blood) • Embolism (downstream travel of a clot) • Infarction (death of tissues w/o blood) • Shock (circulatory failure/collapse)
Platelet disorders • Bleeding disorders.
Normal body composition • Water composes about 60% of total body mass • 2/3 rd of body water is intracellular • 1/3 rd is extracellular
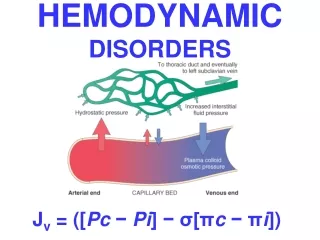
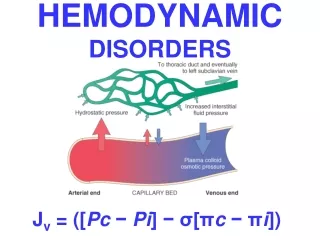
Pathophysiology of Edema Anatomic structures which drain excess interstitial fluid into venous blood: Two opposing major factors governing fluid movement between vascular and interstitial space. Hydrostatic pressure Colloid osmotic pressure
Clinical Correlation • Fluid accumulates in interstitial spaces. • Subcutaneous Edema - RV cardiac & Renal failure • Pulmonary edema in LV failure, • Brain Edema – encephalitis, hypertensive crisis, hydrocephalus, focal injury (Trauma/abscesses/neoplasm)
Clinical manifestations of edema Clinical Signs Most Likely Cause(s)
Pitting Vs Non-Pitting Edema Pitting – Pressing the affected area displaces fluid, leaving a finger shaped depression (pit) that disappears within seconds Non-Pitting – not compressible – caused by chronic lymphedema or myxedema.
Types of exudates • Purulent • Fibrinous • Eosinophilic • Hemorrhagic
Hyperemia and congestion • Increase in blood volume in a particular site. • Hyperemia- active process. Arteriolar dilatation. As seen is acute inflammation, exercising muscle - Redness • Congestion- passive process. Impaired outflow from the tissue. Venous impairment. As seen in congestive heart failure - Cyanosis
Hemodynamic terminology Active congestion • : locally increased blood caused by arteriolar dilation with augmented inflow, as in a working muscle or acute inflammation • : locally increased blood due to impaired venous outflow (lungs in heart failure) Passive congestion Is this hypertrophic liver hyperemic or congested? Nutmeg liver
Active congestion • Vasodilation • By vasoactive mediators • Hormones • Neurogenic effect • Eg-Inflammation • Exercise,blushing • Passive congestion • Decreased venous outflow • CHF • DVT
Hemorrhage • Definition: extravasation of blood because of vessel rupture • Causes: • Mechanical trauma • Atherosclerosis of aorta rupture with acute retroperitoneal hemorrhage • Increased hydrostatic pressure (obstruction or hypertension) • neoplastic erosion of the vessel wall
Nomenclature: hemorrhage Hematoma • : hemorrhage accumulated within a confined space • :1-3 mm hemorrhages skin, mucosa • :3-10 mm hemorrhage skin, mucosa • bruise or echemosis : >1cm hemorrhage skin/subcutis • : hemorrhage into joint Petechie Purpura hemarthrosis
Petechiae, purpuras: small capillary haemorrhages ranging from the size of a pinhead to much larger
Haematomas: may be spontaneous (in a serious hemorrhagic disease) or may occur after trauma (in a mild hemorrhagic disease).
Hemostasis overview • Normal hemostasis • Maintain blood fluid within vessels • Induce rapid localized plug at injury site • Thrombosis • Formation of blood clot within vessel (appropriately or inappropriately) • Three components which regulate normal hemostasis / thrombosis: Vascular wall Platelets Coagulation system
Hemostasis BV Injury Tissue Factor Neural Coagulation Cascade Blood Vessel Constriction Platelet Aggregation Primary hemostatic plug Reduced Blood flow Platelet Activation Fibrin formation Stable Hemostatic Plug • Lab Tests • CBC-Plt • BT,(CT) • PT • PTT Plt Study Morphology Function Antibody
Hemostasis sequence 1 Arteriloar vasoconstriction Prmary hemostasis
Hemostasis sequence 2 Secondary hemostasis Permanent plug formation
NORMAL CLOTTING Response to vessle injury 1. Vasoconstriction to reduce blood flow 2. Platelet plug formation (von willebrand factor binds damaged vessle and platelets) 3. Activation of clotting cascade with generation of fibrin clot formation 4. Fibrinlysis (clot breakdown)
Hemostasis and thrombosis : • Normal hemostasis • A consequence of tightly regulated processes that: • maintain blood in a fluid, clot-free state in normal vessels • inducing the rapid formation of a localized hemostatic plug at the site of vascular injury.
Both hemostasis and thrombosis involve three structural and molecular components: • – the vascular wall • – platelets • – the coagulation cascade
HOMEOSTASIS • Homeostasis which is the property of a system that regulates its internal environment and tends to maintain a stable, relatively constant condition of properties such as temperature or pH.
Thrombosis • Thrombosis: • the pathologic form of hemostasis • involves blood clot (thrombus) formation in uninjured vessels or after relatively minor injury)
Thrombosis can only occur during life • Clotting can also occur after death or in a test tube
Note that: • Hemostasis is a physiological process that occurs during vascular injury to control bleeding normal process. Thrombosis is the pathological counterpart of hemostasis
How normal hemostasis occur ? In 4 steps • 1- Vasoconstriction • 2- Primary hemostasis( control bleeding ) • 3- Secondary hemostasis • 4- Antithrombotic counter regulation • ( control clotting )
1- Vasoconstriction : • After vascular injury, local neuro-humoral factors induce a transient vasoconstriction. It’s a reflex vasoconstriction occurs by secretion of endothelin–a potent vasoconstrictor-
ECM highly thrombogenic sub endothelial extracellular matrix, which is hidden by the endothelium in normal conditions. However, when there is an injury it becomes exposed. It contains vWF (von willebrand) factors and glycoprotein I b (GpIb) receptors.
Platelet secretion (release reaction) • Secretion of granule contentsafter adhesion: • Dense bodies • ADP: promotes aggregation with other platelets • Ionized calcium: enhances coagulation cascade • Thromboxane A2: further aggregation & vasoconstriction • Serotonin, histamine, epinephrine (promoting aggregation & vasoconstriction ) • Activated platelets express surface phospholipid complex, providing binding sites for calcium and factors involved in the intrinsic clotting pathway
2- Primary hemostasis : • Platelets adhere to exposed extracellular matrix (ECM) by binding to vWF (through GpIb receptors) and are activated, undergoing a shape change and granule release. • .
Platelet response to injury • Platelets encounter extravascular matrix molecules: collagen, proteoglycans, fibronectin • Platelets respond in three phases: Platelet adhesion Platelet activation Platelet aggregation
Released adenosine diphosphate (ADP) and thromboxane A2 (TXA2) lead to further platelet aggregation (via binding of fibrinogen to platelet GpIIb-IIIa receptors), to form the primary hemostatic plug.
3- Secondary hemostasis • Endothelial injury also exposes tissue factor (also known as tissue factor III or thromboplstin) a membrane-bound glycoprotein synthesized by endothelial cells. When this factor is released it triggers the coagulation cascade which ultimately leads to activation of thrombin converts fibrinogen into fibrin.
Secundary haemostasis:. • I: fibrinogen • II: prothrombin • III: tissue thromboplastin (tissue factor, TF) • IV: Ca++ • V: Labile factor • VI: -No name • VII: Stable factor • VIII: antihemophilic factor (AHF) • IX: Christmas factor (plasma thromboplastin component) • X: Stuart factor • XI: plasma thromboplastin antecedent (PTA) • XII: Hageman factor (contact factor) • XIII: fibrin stabilizing factor (Laki-Lorand factor)
Local activation of the coagulation cascade (involving tissue factor and platelet phospholipids) results in fibrin polymerization, "cementing"(making it firm) the platelets into a definitive secondary hemostatic plug (larger and more stable )
4- antithrombotic counterregulation • Counter-regulatory mechanisms, such as release of t-PA (tissue plasminogen activator, a fibrinolytic product) and thrombomodulin (interfering with the coagulation cascade–it binds to thrombin and convers it to anticoagulant), limit the hemostatic process to the site of injury
VASCULAR AND PLATELET ABNORMALITIES • Vascular - hereditary • Hereditary hemorrhagic telangiectasia • Ehlers-Danlos syndrome • - acquired • “senile purpura” • Henoch-Schonlein purpura • Scurvy - Amyloid • Steroid purpura
Disorders of the haemostatic mechanism are devided into three main groups: • Disorders of the vessels • Disorders of the platelets • Disorders of the coagulation mechanism (“coagulopathies”) “purpuric diseases”