Download
1 / 20
200 likes | 405 Views
Stenting and Medical Therapy for Atherosclerotic Renal-Artery Stenosis . NEJM, Jan 2014, M Graham-Brown 28/05/14. Background. RAS – present in 1-5% patients with HTN Can also lead to ischaemic nephropathy and ‘flash pulmonary oedema ’ 3 RCT’s show no effect to stenting on BP:

E N D
Stenting and Medical Therapyfor Atherosclerotic Renal-Artery Stenosis NEJM, Jan 2014, M Graham-Brown 28/05/14
Background • RAS – present in 1-5% patients with HTN • Can also lead to ischaemic nephropathy and ‘flash pulmonary oedema’ • 3 RCT’s show no effect to stenting on BP: • van Jaarsveld BC, Krijnen P, Pieterman H, et al. The effect of balloon angioplasty on hypertension in atherosclerotic renal- artery stenosis. N Engl J Med 2000;342: 1007-14. • PlouinPF, Chatellier G, Darné B, Raynaud A. Blood pressure outcome of angioplasty in atherosclerotic renal artery stenosis: a randomized trial. Hyperten- sion 1998;31:823-9. • Webster J, Marshall F, Abdalla M, et al. Randomised comparison of percuta- neous angioplasty vs continued medical therapy for hypertensive patients with atheromatous renal artery stenosis. J Hum Hypertens 1998;12:329-35. • 2 RCT’s show no benefit on progression of CKD: • 15. The ASTRAL Investigators. Revascu- larization versus medical therapy for re- nal-artery stenosis. N Engl J Med 2009; 361:1953-62. • 16. Bax L, Woittiez AJ, Kouwenberg HJ, et al. Stent placement in patients with atherosclerotic renal artery stenosis and im- paired renal function: a randomized trial. Ann Intern Med 2009;150:840-8.
Background • “No studies designed to assess clinical outcomes” • SO… “we performed a randomized clinical trial to determine the effects of renal-artery stenting on the incidence of important cardiovascular and renal adverse events.”
Study oversight • “The Cardiovascular Outcomes in Renal Athero- sclerotic Lesions (CORAL) study was a multi- center, open-label, randomized, controlled trial that compared medical therapy alone with medical therapy plus renal-artery stenting in patients with atherosclerotic renal-artery stenosis and elevated blood pressure, chronic kidney disease, or both.”
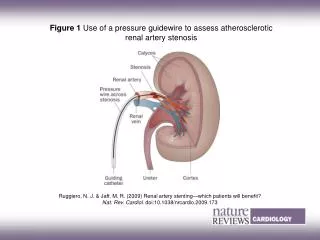
Design and population • Multi-centre • Lead-in period – to ensure the expertise of the lead for IR at each centre • Initially patients with severe RAS were eligible if they had HTN with systolic BP>155mm/Hg on +2 anti-hypertensives • Severe RAS defined as >80%, but <100% OR 60-80% stenosis with a 20mm/Hg systolic pressure gradient
(Re-)design and population • The threshold of 155mm/Hg was no longer specified • Patients who did not have systolic hypertension but who had renal-artery stenosis could be enrolled if they had CKD (eGFR<60) • Severe RAS could be identified using duplex ultrasonography, MRA, or CTA • All changes were made before the trial concluded and/or the results were unblinded
Exclusion criteria • RAS due to fibromusculardysplasia • CKD from a cause other than ischemic ne- phropathy or associated with a serum creatinine level higher than 4.0 mg per deciliter (354 μmol/liter) • Kidney length of less than 7 cm • A lesion that could not be treated with the use of a single stent.
Randomised 1:1 • Medical therapy alone • Anti-platelet, lipid lowering agent, BP medications, glucose (all protocol driven) • Medical therapy + stenting • “Unless otherwise contraindicated, the following medications were mandated by the protocol: the angiotensin II type-1 receptor blocker cande- sartan, with or without hydrochlorothiazide, and the combination agent amlodipine–atorvastatin, with the dose adjusted on the basis of blood pressure and lipid status”
End points • The primary end point was the occurrence of a major cardiovascular or renal event: • Stroke • MI • Hospitalization for congestive heart failure • Progressive renal insufficiency (reduction of 30% from baseline eGFR, sustained for 60 days or more) • The need for permanent RRT
End points • Secondary end-points were death from cardiovascular/renal disease and all cause mortality
Power Calculation • Calculated that 1080 participants would need to be enrolled for the study to have 90% power to test the hypothesis that stenting would reduce the incidence of the primary end point by 25% (hazard ratio, 0.75) at 2 years, at a two-sided type I error rate of 0.05. • Recruitment was slower than anticipated, and terminated after 947 participants had undergone randomization
Stenting and peri-procedural events • The most common angiographic complication was arterial dissec- tion, which occurred in 11 patients • No one in the stent group (or in the medical therapy–only group) required dialysis within 30 days after randomization • One patient (0.2%) in the stent group initiated dialysis between 30 and 90 days after randomization • A patient randomly assigned to medical therapy alone had a fatal stroke on the day of randomization
Blood Pressure • No differences between the groups at end of study • BP declined throughout study period in both groups • No difference in the number of medications they were taking
Conclusions • “The CORAL trial was designed to test whether renal-artery stenting, when added to protocol- driven contemporary medical therapy, improves clinical outcomes in persons with atherosclerotic renal-artery stenosis” • “We found no benefit of stenting with respect to the rate of the composite primary end point or any of its individual components, including death from cardiovascular or renal causes, stroke, myocardial infarction, congestive heart failure, progressive renal insufficiency, and the need for renal-replacement therapy”
Conclusions • “From this result, it is clear that medical therapy without stenting is the preferred man- agement strategy for the majority of people with atherosclerotic renal-artery stenosis”
SO.. • We just have to get the patients to take their medications • #concordance