Download
1 / 14
140 likes | 236 Views
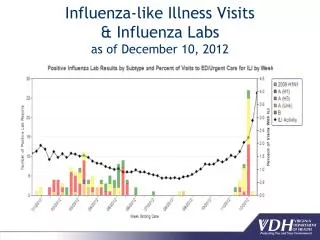
Influenza-like Illness Visits & Influenza Labs as of December 10, 2012. Percent of Flu Doses Administered by Public and Private Sectors, Virginia Influenza Season 2012-13. Source: VIIS and WebVISION data through week ending 12/7/2012, as of 12/11/2012.

E N D
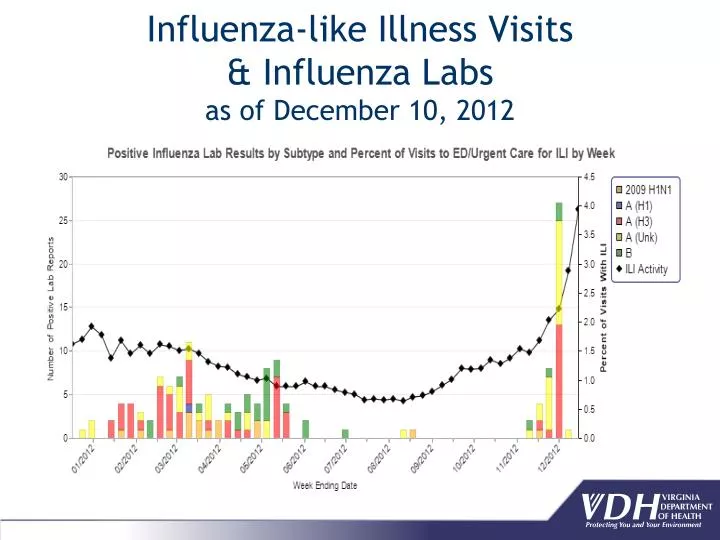
Influenza-like Illness Visits & Influenza Labs as of December 10, 2012
Percent of Flu Doses Administered by Public and Private Sectors, Virginia Influenza Season 2012-13 • Source: VIIS and WebVISION data through week ending 12/7/2012, as of 12/11/2012. • Doses given by the private sector reflect private sector participation in VIIS.
U.S. Influenza Vaccine Virus Strains, 2012-2013 Changes in the A(H3N2) and B strains, compared with last season’s vaccine: • A/Victoria/361/2011 (H3N2)- replaces A/Perth/16/2009 • B/Wisconsin/1/2010 -Yamagata lineage; replaces previous Victoria lineage (B/Brisbane/60/2008) Same: A/California/7/2009 (H1N1)pdm09 • This strain was in in the 2009 monovalent vaccine and the 2010-2011 and 2011-2012 seasonal vaccines
Vaccines Available for 2012-2013 • No new vaccine products anticipated this season • Options similar to last season: • Trivalent inactivated vaccine (TIV/traditional shot) - 6 mos. and older • High dose TIV - 65 yrs. and over • Intradermal TIV - 18 through 64 yrs. • LAIV - healthy, non-pregnant persons 2 through 49 yrs.
Influenza Vaccination Recommendations • Everyone 6 months of age and older is recommended to get the flu vaccine every year • Children 6 months - 8 years of age require 2 doses (administered 4 weeks apart) their first season of vaccination • Vaccination is especially important for people at higher risk of serious influenza complications, or people who live with or care for them
ED/urgent care visits for influenza-like illness (ILI) Laboratory surveillance Sentinel physicians; DFA/PCR/culture by labs Influenza Incidence Surveillance Project (IISP) Weekly activity level reporting (Oct – May) Outbreaks School absenteeism Influenza-associated pediatric deaths Seasonal Flu Surveillance
Districts notified of any suspect novel influenza occurrences should contact DSI immediately. Notify Regional Epi Novel influenza cases are reportable in VA Special case report form Submit specimens for testing; alert DCLS that a novel virus is suspected Novel Influenza Surveillance
Enhanced surveillance for cases of H3N2v this season Patients meeting both of the following criteria should be tested: Fever with cough and/or sore throat (usual ILI definition) Direct contact with swine within the 7 days preceding onset OR an epidemiologic link to a confirmed case of influenza A H3N2v infection If provider interested in testing and/or patient meets criteria: Ask provider to collect NP swab, place in viral transport media (or provide a DCLS flu test kit to them) and complete DCLS specimen submission form Note outbreak ID: RES989H3N2vSurv12 on the DCLS form Confer with DSI, through regional epidemiologist to be sure there is agreement patient warrants testing and ensure that DCLS knows a specimen is on the way Submit the specimen to DCLS Novel Influenza Surveillance: H3N2v
West Nile Virus (WNV) Update • Nationwide WNV disease activity is greater than it has been since the mid 2000s • As of Dec. 10th, WNV disease has been reported in 29 Virginians from all five health regions of the state • Three WNV-related deaths in Virginia • Neuroinvasive disease reported in 21/29 (72%) • Last year, 9 reports of WNV disease in Virginians • For 2006 to 2010, 1-5 WNV reports annually • Best way to avoid WNV is to prevent mosquito bites • Use insect repellent, consider staying indoors during dusk and dawn, use good screens on windows, empty containers/pools with standing water
Other Human Arbovirus Activity, 2012 • Eastern Equine Encephalitis (EEE) reported in one Virginian • Portsmouth HD • Not a death • First human case of EEE reported in Virginia since 2003 • La Crosse Encephalitis (LAC) reported in two Virginians • Both Lenowisco HD • No deaths • Virginia reported one case of LAC disease in 2011 and two cases in 2008
Fungal Meningitis Investigation – First Steps • Notified by CDC on evening of September 29, 2012 of cases of fungal meningitis potentially associated with exposure to contaminated epidural steroid injections • Steroids were from three recalled lots of product manufactured by the New England Compounding Center • Two locations received these products in Virginia – New River Valley Surgery Center and Insight Imaging Roanoke • Facilities gave VDH patient lists so that each could be contacted to inform them of their potential exposure and ask about symptoms. Facilities also contacted patients themselves. • Letter sent to SW physicians on October 1.
Fungal Meningitis Investigation – Two Key Categories of Response • Surveillance of Exposed • 680 exposed to recalled lots of MPA in VA facilities • ~95% at Roanoke facility • Reside in 10 VA health districts plus 4 other states • Health departments called weekly unless the person under doctor’s continuing care for this outbreak • Case Finding and Reporting • 51 cases, 2 deaths as of December 10, 2012 • Median age 64 years; all hospitalized • Working closely with hospitals – infectious disease specialists, laboratories, infection prevention
Fungal Infections among Patients Exposed in Virginia by Date of Onset (as of December 10, 2012, n=51)
Fungal Meningitis Investigation –Key Public Health Activities • Coordination and communication • Local, state, and federal health agencies • Public health and clinical community • Local health department surveillance and case reporting • Regional/central office epidemiologists compiling & verifying detailed information, working with DCLS, and reporting to CDC • Central office staff deployed to the region • CDC Epi-Aid deployed to Virginia – clinical assessment • Clinician letters and conference calls