Download
1 / 20
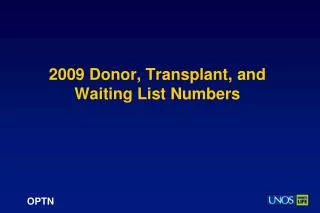
200 likes | 365 Views
Expanding the Donor Pool: ECD and DCD Practice. Carl-Ludwig Fischer-Fröhlich, Stuttgart, Germany. Expanded criteria donors (ECD). frequent co-morbidities in donors donor derived diseases transmission Mortality / Morbiditiy pitfalls . infection. malignancy. poisoning.

E N D
ExpandingtheDonor Pool:ECD and DCD Practice Carl-Ludwig Fischer-Fröhlich, Stuttgart, Germany
Expanded criteria donors (ECD) • frequent co-morbidities in donors • donor derived diseases transmission Mortality / Morbiditiy • pitfalls infection malignancy poisoning gene defect • acute – chronic – latent – cured – recurrence free ? • global or local problem ? • treatment in the recipient possible ? • benefit for the individual recipient ?
Example: 52 yrs, SAH (admitted 10 h after event) Brain death and Inflammation: • Infection parameters: = become unreliable • brain injury • brainstem coning • overlay of infection ??
Infections (1) Critical Symptoms • Previous mental or neurological changes(skin / fever / diarrhea / pain / body examination): • poisoning? malignancy? exotic virus – fungus – bacteria – parasite - zoonosis? • Living conditions / social situation / „antecedents“: • chance for collecting infectious pathogens • traveling, working, living, pets, animals, sanitary condition, CDC-risk • Diagnostic tests may fail ! • serology, cultures, PCR etc.: specific / sensitive? false pos./neg. ? • Minimum screening (serology +/-PCR if indicated in high risk population): • HIV, Hepatitis B & C, CMV, EBV, Toxoplasmosis • Further pathogens according to regional prevalence (WMV, Dengue, Malaria…) Council of Europe: Guide to the safety and quality of organs in transplantation of organs (5th ed., 2013)
Infections (2) systematic spread / blood = transmission latent / locally restricted = different patterns of transmission (e.g. CMV) properly treated infection = no exclusion (e.g. 48h antibiotics in bacteria) communicate all in coming results / data to recipient centers reassess with recipient CMV-, PCP-, antibiotic-prophylaxis et al. Absolute Contraindication: Encephalitis or Meningitis of unknown origin Un-treated true Sepsis or tuberculosis Bacteria, Virus, Fungus, Parasites et al.: Council of Europe: Guide to the safety and quality of organs in transplantation of organs (5th ed., 2013)
Malignancy staging TNM – histology – therapy – recurrence free – kind of follow up brain tumor vs. other solid tumors vs. haematopoetic disorders tumor markers: not reliable transmission risk assessment: Transplant Registries (e.g. UNOS / IPTTR), case reports: low rate of transmission if donor was properly screened lethal adverse events if overseen in donor current practice:~ non cerebral: some T1N0M0, if recurrence free survival > * years~ cerebral: WHO Grade + duration + therapy Final decision depends on recipient’s needs …but never forget to screen for malignancy in a potential donor Council of Europe: Guide to the safety and quality of organs in transplantation of organs (5th ed., 2013)
Gene Defector rare diseases Donor 73 yr., cerebral stroke -> bleeding Glycogenosis Type 5 (Mc Ardle): - gene 11q13 defect for muscle-myophosphorylase - isoenzyme for liver and brain coded by other gene - risk for rhabdomyolysis after severe exercise www.orphanet.net Glycogenosis Council of Europe: Guide to the safety and quality of organs in transplantation of organs (5th ed., 2013)
Poisoning CO and / or Cyanide (smoke) • Check fordetoxicationandrecoveryfrompoisoning Council of Europe: Guide to the safety and quality of organs in transplantation of organs (5th ed., 2013)
- 100 kg, 170cm, ICB, untreated hypertension, smoker, alcohol, - ICU-Nurse: “Hi, needs volume and MAP >75 for diuresis, Crea. normal” prevention of acute kidney injury (with assumed chronic damage) liver-fibrosis, 3 vessel-CAD, arteriosclerosis both kidneys had primary function Preservation of organ function before recovery… Donormaintenanceimproves marginal organs !
…pitfalls at recovery Final check in thoraxandabdomen !
Is it safe to use this liver for transplantation? • 67 years SAH • ICU = 17 days • ALAT = 91 IU/l • BMI = 35 kg/m² • paO2/FIO2= 134 • Diabetes Typ II • Hypertension • Tetanus as child • anti-HBc +, HBsAg - 5% macrovesiuclar steatosis,slight choelstasis, slight cholangitis Consensus: Qualified examination at recovery + biopsy + care for HBV-transmission
Liver: Interaction donor & ECD & recipient Donor: Age Recipient: Co-Morbidity (age) + actual status (Bili, Crea, HU) EDC are not relevant after proper donor selection Frühauf NR, Fischer-Fröhlich CL, Kutschmann M, Schmidtmann I, Kirste G. Transplantation, 2011 ; 92: 1378-1384
Kidney: donor age = ECD ? (Germany 2009-2012, n=7309, courtesy DSO/Aqua) Graft survival rate (p < 0,0001): Death censored graft survival rate (p < 0,0001): Days after transplantation Days after transplantation Donorageexplaining variable in all COX regressions in German population
The Brain - Heart Connection: Poor cardiac output mitigated byinotropic support (dobutamine)after stress cardiomyopathy Donor chatecholamine support heart transplantion *1- if (after SAH/ICB) primary graft failure *2- if (at vasoplegia) no effect on graft function Peripheral vasoconstriction afterbrain death (norepinephrine) *3 Experiment:explosive ICP ~ irreversible myocard damage~ contraction band necrosis *5 SAH cardiac failure ~ cardiac function workup *6 avoid at brain stem coning ~ by Esmolol or Urapidil *4Stress related cardiomyopathy: …acute stress , severe illness or …”sudden intracranial disease” ~ explosive catecholamine release at nerve ends of myocard ~ arrythmia, akinesia, LVF… *7 after brain stem coning ~ donor resucitation protocol (covers other pathologies) *1Santise, InteractCardiovascSurg 2009, 9, 476-479 *2 Silva, Intens Care Med, 2002, 28, Suppl. 66 *3Shivalkar, Circulation 1993, 87, 230-239 *4Bybee, Prasa, Circulation 2008, 118, 397-409 *5 Lee NeuroCrti Care 2006,5, 243-249 *6 Mertens, Organs Tissues Cells 2007, 10, 159-165 *7Zaroff, Ciruclation 2002, 106, 836-841
DCD categories: Kootstra G, Daemen JH, Oomen AP. 1995. Categories of non-heart-beating donors. Transplantation Proceedings 27(5):2893–2894.
DCD: some basics • How do you confirm death after the terminal cessation of heart function ? • Does this DCD concept fit your legislation about brain death diagnostics ? • How complies your no-touch period with the ”Donor Dead Rule“ ? • Is DCD accepted within your health care system ? • You must have a convinced team with all partners in the hospital integrated ! • You must have an effective protocol for all steps in your hospital ! • Example Germany: • in every donor death & irreversible cessation of all brain functions must be confirmed before an organ can be recovered for transplantation after consent. • any no-touch-period does not confirm this as safe sign of death……
Controlled DCD • If all ok: apply your protocol (e.g.) • prepare recovery • prepare WLST • Consider farewell • Perform WLST • In case of cardiac arrest <120’ proceed with recovery after appropriate no-touch period forassuring irreversible cardiac arrest otherwise stop procedure • Keep ischemia times low • Select appropriate recipients • Compensate side effects of pro-longed warm ischemia by proper organ preservation • Results might be equivalent to DBD when performed properly.
uncontrolled DCD • Apply protocol consented with all partners in your healthcare system: • CPR failed, usually otherwise healthy persons (outside/inside hospital) • Rapid arrangements in your hospital (unexpected event) • Death certification by team independent from recovery or transplantation • Appropriate family approach (time constraints) • If consent farewell & recovery (see controlled DCD) or otherwise stop • Critical issue: • Some maneuvers mandatory pre-consent & CPR continued until… et al.
Expanding the donor pool: ECD and DCD practice Conclusion: Case wise decision • Expanded donor criteria~ risk for compromised grafts • Restricted donor criteria~ dead on waiting list anyway • Personal alert: - “I may oversee a donor”- fit recipient to donor- update protocols (research) • Thank you