Download
1 / 25
250 likes | 579 Views
Respiration and The Complications of a Ventricular Septal Defect (VSD). Gregg McCord, MS Penn State Hershey, MSII. Learning Objectives: . I: Understand the basic function of our lungs II: Understand how blood is carried to our tissues

E N D
Respiration and The Complications of a Ventricular Septal Defect (VSD) Gregg McCord, MS Penn State Hershey, MSII
Learning Objectives: • I: Understand the basic function of our lungs • II: Understand how blood is carried to our tissues • III: Correlate VSD and how this affects respiration and delivery of oxygen to our tissues • IV: Know what factors help determine the severity of a VSD • V: When you would treat a child with this condition.
What are the functions of the Lungs? (There are Two Main Things) • 1. DELIVER OXYGEN TO OUR BLOOD! (Inhalation) • 2. TAKE CARBON DIOXIDE OUT OF OUR BLOOD! (Exhalation) • How do we do this?
Red Blood Cells!! The pack mule of the body • Make Up 40% of our total blood volume. • They can bind to Oxygen and unbind Oxygen. • They can bind Carbon Dioxide and unbind Carbon Dioxide • They are flexible and can fit through tight spaces • They are durable and long lasting (120 days!!)
Storage Available!! • The RBC’s contain a special molecule called Hemoglobin. • Hemoglobin loves Oxygen but at the same time is not terribly picky, and is willing to hold onto Carbon Dioxide in the event that oxygen leaves to be used by the tissues. Hemoglobin O2 CO2
RED CELLS RESPOND TO PEER PRESSURE 1 2 3 O2 CO2 4 CO2
Summary of Last Slide • 1. Blood Is pumped to the lungs from the Right Ventricle thru the pulmonary artery while person is inhaling. • O2 pressure High and CO2 Pressure Low in the lungs • RBC gives CO2 to Lungs in exchange for O2 O2 CO2 O2
Summary Continued… 2. Blood Leaves the lungs and enters the left atrium and ventricle from the pulmonary veins • Oxygenated blood carried by RBC’s is ejected from the left ventricle to enter arteries and be carried to the body where tissues are doing work and using oxygen. • RBC’s with High oxygen pressure let go of Oxygen while tissues with high CO2 release CO2 into the blood and RBC’s pick this up and carry it back to the heart.
So who cares about Oxygen? It is our main source of energy and is important for many biological reactions. Without it we are not able to carry out our bodies normal metabolic functions. What are some symptoms that you might expect from someone who has decreased abilities to carry oxygen to their tissues? Think about your patient… Before we answer this question in its entirety we need to think about how the heart is important for delivery of oxygenated blood after the lungs have done their part.
Bring it back to the heart of things… Right vs. Left Heart • Right side pumps to the lungs so does not need as much force production in comparison to the Left side which needs to pump to the entire rest of the body!!!
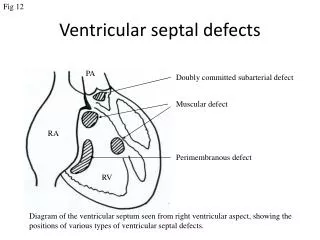
Muscle and Finesse… • Shaq = The Left Ventricle • Kobe = the Right Ventricle • As long as they are divided from one another by a wall (septum) they really don’t care. What happens however when there is a hole in that wall?
Why would this be bad? • 1. Decreased blood going out to the body! • 2. The right and left ventricle are having to work a lot harder and are deforming to do so. • 3. The pulmonary circulation does not normally handle this large increase in blood.
1. Decreased blood (cardiac output) going out to the body! • Adaptation: • How do you think the heart will compensate? • Would you expect growth in an infant to be normal if they had this condition? Why might this be? • Would you expect there to be a murmur present? During what part of the cardiac cycle?
2. The right and left ventricles are having to work a lot harder
3. The pulmonary circulation does not normally handle this large increase in blood. • Adaptation: • Increased pulmonary vascularization (blood vessels) • Pulmonary Edema (leakage) causing abnormal breath sounds
CONGESTIVE HEART FAILURE! • This may be the end result of a VSD if it goes untreated. The back of blood into the heart and failure to pump the blood properly through the lungs can lead to leakage of fluid (congestion) and eventual failure of the heart muscle to pump adequate blood out to the tissues (heart failure). • Intervention should occur before this condition occurs because of a VSD.
Symptomology of Allen • Do the symptoms add up with someone who has a VSD and why? • Allen’s Symptoms: • Left Ventricular enlargement? • Increased pulmonary vascularization? • Extreme cardiomegaly, especially in the area of the right atrium? • Increased Pulse • Abnormal Growth
Treatment • What do you do if you have a hole in your bucket? What if it is a small hole that barely leaks any water at all? What if it is a large hole?
VSD Treatment • Small VSD: • Usually treated conservatively with watchful waiting, and many times as the heart grows, the VSD will spontaneously resolve. If not then it is treated with drugs to help decrease the work that the heart has to do.
Long Term Outlook • EXCELLENT!! • Long term survival without incidence is great in children treated • Most survivors lead asymptomatic lives with the tendency to have slightly lower exercise capacity.