Download
1 / 19
220 likes | 528 Views
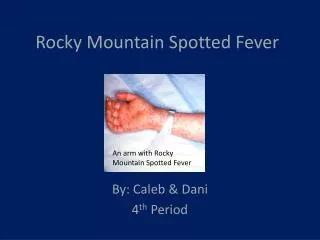
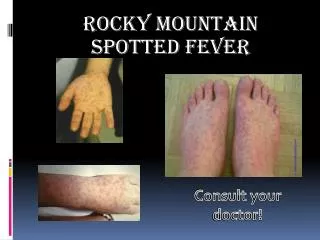
Rocky Mountain Spotted Fever. Rocky Mountain Spotted Fever:. First recognized in 1896 in the Snake River Valley of Idaho and was originally called "black measles" because of the characteristic rash.

E N D
Rocky Mountain Spotted Fever: • First recognized in 1896 in the Snake River Valley of Idaho and was originally called "black measles" because of the characteristic rash. • Howard T. Ricketts established the identity of the infectious organism that causes this disease, Rickettsia rickettsii. • He and others described the epidemiologic features of the disease, including the role of tick vectors. • Sadly, Dr. Ricketts died of typhus (another rickettsial disease) in Mexico in 1910.
Epidemiology: • A bit of a misnomer, this disease has been identified in almost all of the continental US, with perhaps the exception of Maine and Vermont • Most cases reported in south Atlantic, southeastern and south central states • 54% of cases were from NC, TN, OK, SC and Ark
Transmission: • Vector=tick • Wood tick, dog tick and Lone Star tick • Both dog and Lone Star ticks are found in NC • Wood tick is primarily in western US, and Rocky Mountain area
DOG TICK: Transmits RMSF, but probably not Lyme • LONE-STAR TICK: Transmits RMSF, and human monocytic ehrlichiosis
Two-thirds of RMSF cases occur in children younger than 15 years • Males are infected more commonly (1.7-2.2:1) • Caucasians are more common than African-Americans • Peak months of infection are April-October
R. rickettsii organisms are released through saliva during a feeding • Usually 12-24 hrs of attachment is required • Incubation period is 2-14 days • Once organisms enter the body, they multiply within endothelial cell linings of small blood vessels
Signs and Symptoms: • EARLY: • Fever, nausea, vomiting, severe headache, anorexia and malaise • LATE: • Rash, joint pain and diarrhea • Classic triad=fever, rash and headache • Rash: appears between day 2 to 5 of illness • Blanching, erythematous macules arouond ankles feet, later wrists and hands; palms and soles often involved • Petechiae on day 6 • 10-15% of infected patients are without rash
Important points: • Only 40-60% of those infected have a history of tick bite • RMSF may be clinically indisginguishable from Human Monocytic ehrlichiosis
Laboratory tests: • Hyponatremia (20%) • Thrombocytopenia (33%) • Anemia, increased LFTs or BUN (25%) • CSF: monocytic pleocytosis, increased protein
Diagnosis: • Largely clinical • Suspect if classic triad • Acute and convalescent titers (> 3 wks apart) • Immunofluorescence assay • PCR • Isolation of R rickettsii from clinical specimen
Treatment: • Should be started immediately • Doxycycline, usually 7-10 days • 100 mg PO BID for adults • 4 mg/kg/day div BID for children • Discontinue 72 hrs after defervescence • Teeth staining if < 9 years old; probably requires 5-6 courses before staining appears
Prevention: • Protective clothing • Repellants • Avoid DEET if under 12 months • Full body examinations
To remove attached ticks, use the following procedure: • 1. Use fine-tipped tweezers or shield your fingers with a tissue, paper towel, or rubber gloves (Figure 17). When possible, persons should avoid removing ticks with bare hands. • 2. Grasp the tick as close to the skin surface as possible and pull upward with steady, even pressure (Figure 18). Do not twist or jerk the tick; this may cause the mouthparts to break off and remain in the skin. (If this happens, remove mouthparts with tweezers. Consult your health care provider if infection occurs.) • 3. Do not squeeze, crush, or puncture the body of the tick because its fluids (saliva, body fluids, gut contents) may contain infectious organisms. • 4. After removing the tick, thoroughly disinfect the bite site and wash your hands with soap and water. • 5. Save the tick for identification in case you become ill. This may help your doctor make an accurate diagnosis. Place the tick in a plastic bag and put it in your freezer. Write the date of the bite on a piece of paper with a pencil and place it in the bag.
Resources: • Center for Disease Control and Prevention. Rocky Mountain spotted fever. Available at: http://www.cdc.gov/ncidod/dvrd/rmsf • Pickering, L. Red Book; 26th edition. pp. 532-534. • Razzaq, S. Rocky Mountain Spotted Fever: A Physician’s Challenge. Pediatrics in Review. Vol. 26, No. 4 April 2005. pp. 125-129.