Download
1 / 9
100 likes | 376 Views
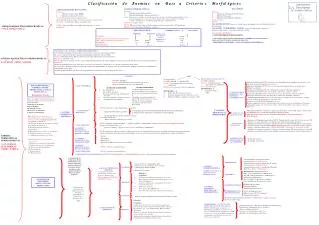
ANEMIAS MICROCÍTICAS GENERALMENTE HIPOCRÓMICAS MARÍA ESTHER DESCHAMPS LAGO. G L O B I N A S. H E M E. TALASEMIAS. P R O T O P O R F I R I N A. Fe. ANEMIAS SIDEROBLÁSTICAS. RELATIVAS

E N D
ANEMIAS MICROCÍTICAS GENERALMENTE HIPOCRÓMICAS MARÍA ESTHER DESCHAMPS LAGO
G L O B I N A S H E M E TALASEMIAS P R O T O P O R F I R I N A Fe ANEMIAS SIDEROBLÁSTICAS RELATIVAS ANEMIA DE ENFERMEDADES CRÓNICAS: EL HIERRO SE ENCUENTRA SECUESTRADO EN LOS MACROFAGOS POR AUMENTO EN LA PRODUCCIÓN DE NFT (FACTOR DE NECROSIS TUMORAL), QUE CONDUCE A MAYOR PRODUCCIÓN DE FERRITINA-L (HEPÁTICA) QUE LIBERA POCO HIERRO. ABSOLUTAS ANEMIA POR DEFICIENCIA DE Fe
ANEMIAS MICROCÍTICAS HIPOCRÓMICAS: VGM HCM CMHG • ANEMIAS POR DEFICIENCIA DE FE. • Mecanismos: • Deficiente síntesis de grupo HEME. • Deficiente producción de eritrocitos • Causas:Deficiencia nutricional y sangrado crónico. • (En el sangrado agudo, la anemia es más bien normocítica, normocrómica.) • Reticulocitos: normales. En respuesta a tratamiento::altos • FROTIS: Anisocitosis, Microcitosis, Hipocromía, eliptocitos, codocitos, poiquilocitos.
Paciente Normal Fe Sérico: 100g CTFT: 300g IST: 300 X 100 = 33.3% 100 N= 20 - 50% Fe sérico 50-150g/dL CTFT 300-360 g/dL Ferritina sérica 50-200g/L IST 20-50% Hemosiderina +++
DEFICIENCIA DE Fe SIDEROBLÁSTICAS Y TALASEMIAS ABSOLUTA RELATIVA Fe SÉRICO: Normal ó CTFT (Capacidad Total de Fijación de Transferrina ): Normal IST(Indice de Saturación de Transferrina ): <10% 10-20% > 20 FERRITINA <12 20-200 > 50 HEMOSIDERINA 0 + A ++++ Normal ó Anemias de los Padecimientos Crónicos Inflamatorios e Infecciosos.
ANEMIAS SIDEROBLÁSTICAS • Mecanismos: • Deficiente síntesis de Protoporfirina. • Hemólisis Intramedular ( eritropoyesis ineficaz) • Causas: Deficiencias hereditarias de enzimas que afectan la síntesis de la Protoporfirina;Inhibici´n de las mismas enzimas por intoxicación por Plomo, Etanol ( Otra causa de anemiea en el enfermo cirrótico), Cloramfenicol; en la Mielodosplasia Tipo II y en Eritroleucemia. • Reticulocitos: normales ó bajos. • FROTIS: Microcitosis, hipocromía, moderada poiquilocitosis, anisocromía, cuerpos de Pappenheimer. • MEDULA OSEA: Sideroblastos Patológicos ( en anillo )
TALASEMIAS Mecanismos: Deficiencia Hereditaria de Síntesis Globinas Hemólisis Intravascular Hemólisis intramedular Beta-Talasemias Reticulocitos: altos FROTIS: TALASEMIA MENOR: microcitosis notable, hipocromía mínima, codocitos. Punteado basófilo en Beta talasemias. TALASEMIA INTERMEDIA Y MAYOR: microcitosis, hipocromía, poiquilocitos talasémicos ( hipocrómicos ), eritroblastos, punteado basófilo. DIAGNÓSTICO DEFINITIVO: 1) ELECTROFORESIS DE HEMOGLOBINA. 2) INDUCCIÓN Y BUSQUEDA DE PRECIPITADOS DE HbH EN AZUL DE CRESILO BRILLANTE DESPUÉS DE 1 HORA DE INCUBACIÓN: ENFERMEDAD POR HbH(ALFA TALASEMIA INTERMEDIA )