Download
1 / 1
40 likes | 222 Views
Go Aphasia!: Examining the efficacy of Constraint-Induced Language Therapy for agrammatic aphasia Christine Virion & Yasmeen Faroqi-Shah University of Maryland, College Park. Protocol. Discussion. Background. o-CILT produced limited gains, hence:

E N D
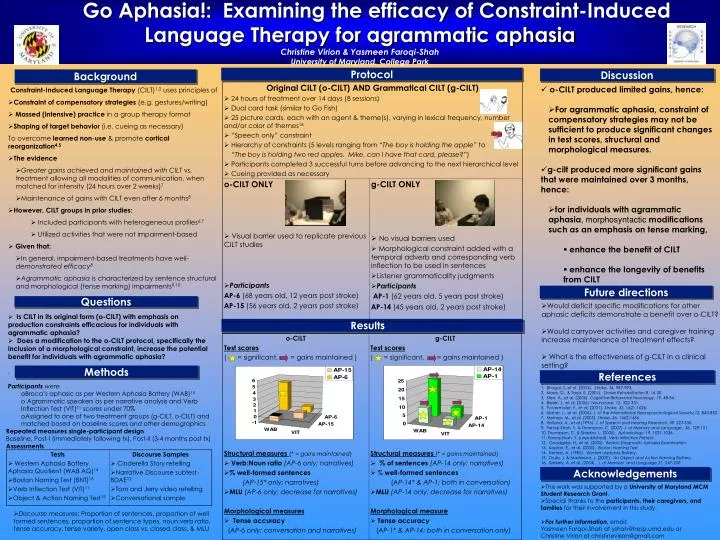
Go Aphasia!:Examining the efficacy of Constraint-Induced Language Therapy for agrammatic aphasia Christine Virion & Yasmeen Faroqi-Shah University of Maryland, College Park Protocol Discussion Background • o-CILT produced limited gains, hence: • For agrammatic aphasia, constraint of compensatory strategies may not be sufficient to produce significant changes in test scores, structural and morphological measures. • g-cilt produced more significant gains that were maintained over 3 months, hence: • for individuals with agrammatic aphasia, morphosyntactic modifications such as an emphasis on tense marking, • enhance the benefit of CILT • enhance the longevity of benefits from CILT • Constraint-Induced Language Therapy (CILT)1,2 uses principles of • Constraint of compensatory strategies (e.g. gestures/writing) • Massed (intensive) practice in a group therapy format • Shaping of target behavior (i.e. cueing as necessary) • To overcome learned non-use &promote cortical reorganization4,5 • The evidence • Greater gains achieved and maintained with CILT vs. treatment allowing all modalities of communication, when matched for intensity (24 hours over 2 weeks)7 • Maintenance of gains with CILT even after 6 months8 • However, CILT groups in prior studies: • Included participants with heterogeneous profiles6,7 • Utilized activities that were not impairment-based • Given that: • In general, impairment-based treatments have well-demonstrated efficacy8 • Agrammatic aphasia is characterized by sentence structural and morphological (tense marking) impairments9,10 Future directions Questions • Would deficit specific modifications for other aphasic deficits demonstrate a benefit over o-CILT? • Would carryover activities and caregiver training increase maintenance of treatment effects? • What is the effectiveness of g-CILT in a clinical setting? • Is CILT in its original form (o-CILT) with emphasis on production constraints efficacious for individuals with agrammatic aphasia? • Does a modification to the o-CILT protocol, specifically the inclusion of a morphological constraint, increase the potential benefit for individuals with agrammatic aphasia? • . Results Methods References • Participants were • Broca’s aphasic as per Western Aphasia Battery (WAB)14 • Agrammatic speakers as per narrative analysis and Verb Inflection Test (VIT)11 scores under 70% • Assigned to one of two treatment groups (g-CILT, o-CILT) and matched based on baseline scores and other demographics • Repeated measures single-participant design • Baseline, Post-I(immediately following tx), Post-II(3-4 months post tx) • Assessments • Discourse measures: Proportion of sentences, proportion of well formed sentences, proportion of sentence types, noun:verb ratio, tense accuracy, tense variety, open class vs. closed class, & MLU • Bhogal, S.,et al. (2003). Stroke, 34, 987-993. • Morris, D., & Taub, E. (2001). Stroke Rehabilitation 8, 16-30. • Sterr, A., et al. (2006). Cognitive Behavioral Neurology, 19, 48-54. • Breier, J., et al. (2006). Neurocase, 12, 322-331. • Pulvermuller, F., et al. (2001). Stroke, 32, 1621-1626. • Maher, L., et al. (2006). J. of the International Neuropsychological Society,12, 843-852. • Meinzer, M., et al. (2005). Stroke, 36, 1462-1466. • Holland, A., et al.(1996). J. of Speech and Hearing Research, 39, S27-S36. • Faroqi-Shah, Y. & Thompson, C. (2007) J. of Memory and Language , 56, 129-151. • Thompson, C. & Shapiro, L. (2005). Aphasiology, 19. 1021-1036. • Faroqi-Shah, Y. (unpublished). Verb Inflection Pretest. • Goodglass, H., et al. (2000). Boston Diagnostic Aphasia Examination. • Kaplan, E., et al. (2000). Boston Naming Test. • Kertesz, A. (1982). Western Aphasia Battery. • Druks, J. & Masterson, J. (2000). An Object and Action Naming Battery. • 16. Szekely, A. et al. (2004). J. of Memory and Language,51, 247-250. Acknowledgements • This work was supported by a University of Maryland MCM Student Research Grant. • Special thanks to the participants, their caregivers, and families for their involvement in this study. • For further information, email: Yasmeen Farqoi-Shah at yshah@hesp.umd.edu or Christine Virion at christinevirion@gmail.com