Download
1 / 60
680 likes | 1.13k Views
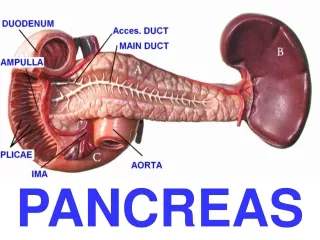
TUMORE DEL PANCREAS. Stefano Cereda Dipartimento Oncologico Ospedale S. Raffaele - Milano. RICHIAMI ANATOMICI. EPIDEMIOLOGIA. EPIDEMIOLOGIA. CARCINOMA PANCREATICO Quarta causa di morte per tumore Responsabile del 5% delle morti per tumore 50000 morti/anno in Europa

E N D
TUMORE DEL PANCREAS Stefano Cereda Dipartimento Oncologico Ospedale S. Raffaele - Milano
CARCINOMA PANCREATICO Quarta causa di morte per tumore Responsabile del 5% delle morti per tumore 50000 morti/anno in Europa 28000 morti/anno negli USA
malattia dell'anziano: circa 80% dei pazienti ha tra 60 e 80 anni e < 2% meno di 40 anni lieve prevalenza per il sesso maschile. Fattori ormonali responsabili della crescita neoplastica
Normal PanIN-1A PanIN-1B PanIN-2 PanIN-3 Oncogene activation Loss of tumor suppressor genes Pancreatic cancer progression Hruban et al
Factors Associated with Increased Risk of Pancreatic Ca. Advancing age African American males Low socioeconomic status Native female Hawaiians Ashkenazi Jewish heritage Cigarette smoking Six genetic syndromes Diabetes mellitus Chronic pancreatitis Cirrhosis Obesity Increased height Low level of physical activity High-fat and cholesterol diet Occupational exposure to carcinogen
Genetic Syndromes and Gene Alterations Associated with Familial Pancreatic Cancer Syndrome Hereditary pancreatitis PRSSI (7q35) Hereditary nonpolyposis colorectal ca (Lynch II variant) hMSH2, hMLH1, others Hereditary breast and ovarian ca. BRCA2 (13q12q13) Familial atypical multiple mole melanoma (FAMMM) syndrome p16 (9p21) Peutz-Jeghers syndrome STK11/LKB1 (19p13) Ataxia-telangiectasia ATM (11q22-23)
EZIOLOGIA • RAZZA: non esistono dati univoci • FAMILIARITÁ: Ruolo non chiarito. La reale importanza potrà essere apprezzata se i difetti genetici saranno identificati • FATTORI AMBIENTALI-OCCUPAZIONALIlavorazione del DDT: Rischio Relativo aumentato di 7 volte e correlato con durata dell'esposizione e dose
SINTOMATOLOGIA Il carcinoma del pancreas è frequentemente sintomatico.La mancanza di specificità di alcuni di questi sintomi è causa di ritardata diagnosi.
L'approfondimento diagnostico strumentale è condizionato da: • finalità diagnostica e stadiazione • disponibilità strumentale • expertise disponibili
Ecografia addome • TAC • RMN • esami ematochmici • PET • Ecoendoscopia/ERCP • Laparotomia
Ca 19.9: il più usato ed il più specifico. Può non essere espresso in relazione alla negatività dell'antigene di Lewis. Alti livelli possono essere condizionati dalla presenza di colostasi CAM 17-1: alta sensibilità e specificità con un buon valore predittivo sia per il positivo che per il negativo CEA: bassa sensibilità, specificità e VPP. Accuratezza diagnostica che non supera il 67% DUPAN-2, CA50: poco utilizzati con indici di sensibilità e specificità di poco superiori al CEA
DIAGNOSI E STADIAZIONE PRESENZA / ASSENZA LESIONE CRITERI OPERABILITA’ (soggettivi) • coinvolgimento strutture circostanti • coinvolgimento strutture vascolari • metastasi a distanza
STADIO T1Tumore < 2 cm T2Tumore > 2 cm T3Tumore esteso oltre il pancreas ma senza infiltrazione del tripode celiaco o dell’arteria mesenterica superiore T4Tumore infiltrante il tripode celiaco o l’arteria mesenterica superiore N1a Interessamento di un linfonodo regionale N1b Interessamento di più linfonodi regionali
STADIO IA T1 N0 M0 IB T2 N0 M0 IIA T3 N0 M0 IIB T1-3 N1 M0 III T4 N0-1 M0 IV T1-4 N0-1 M1
Adenocarcinoma of the pancreas is the deadliest of all of the cancers
PRINCIPI di TERAPIA stadio IA-IIB (III)
CHIRURGIA RADICALE l'approccio chirurgico rappresenta un tempo fondamentale
CHIRURGIA RADICALE per i tumori della testa del pancreas prevede la duodenocefalopancreasectomia secondo Whipple o secondo Longmire-Traverso (conservazione del piloro) La chirurgia del corpo e coda prevede la spleno-pancreasectomia distale Queste metodiche possono essere accompagnate o meno da linfoadenectomia allargata
FATTORI PROGNOSTICI • Centro • Stadio • Grading (G3) • Dimensioni (> 3 cm) • PS • CA19.9 • Margini di resezione (R0-R1-R2) (?) • Sede ?
PANCREATIC SURGERY MORTALITY FOR PANCREATO-DUODENECTOMY Low-volume hospital: 16.3% High-volume hospital: 3.8% Definition of highvolume hospital: at least 16 PD / year N Engl J Med 2002
CHIRURGIA RADICALE Chirurgia sola 12 mesi mortalità 2-16%
PATTERN OF FAILURE • local failure 25-62% • isolated local failure 0-35% • distant failure 51-79% • early failure (<6 mo) 90% distant
RADIOTERAPIA L’impiego postoperatorio della radioterapia è giustificato dall’elevato rischio di recidiva locale
PATTERN OF FAILURE • local failure 25-62% • isolated local failure 0-35% • distant failure 51-79% • early failure (<6 mo) 90% distant
CHEMOTHERAPY Survival 2-year 5-year No CHEMO: 30% 8% CHEMO: 40% 21% HR=0.71 (0.55, 0.92), p=0.009 5FU 425 mg/m2 LV 20 mg/m2 x 5d every 4 w Neoptolemos NEJM 2004
p= 0.001 ADJUVANT CHEMOTHERAPY • Gemcitabine mDFS 14.2 mo. • Observation mDFS 7.5 mo. Neuhaus ASCO 2005
WHAT DID WE LEARN ? • surgery alone is inadequate • micrometastases occur often & early • systemic therapy as 1st postop treatment • local failure is the rule • consider chemoradiation • nearly every case is candidate for a multimodal approach
PRINCIPI di TERAPIA stadio III
LOCALLY ADVANCED DISEASE NEARLY ALL PATIENTS DEVELOP METASTATIC DISEASE • early stage systemic therapy • advanced stage local therapy ???? CHEMO SHOULD ALWAYS BE THE 1st TREATMENT
N=72 chemoRT mOS 15 mo. N=56 further chemo mOS 12 mo. N=53 PD chemochemoRT vs chemo PHASE II TRIALS – STAGE III chemo x 3 cycles (various regimens) p=0.0009 GERCOR - ASCO 2005