Download
1 / 49
510 likes | 739 Views
Towards a UK Charged Particle Research Facility. Bleddyn Jones MD Gray Institute for Radiation Oncology and Biology, University of Oxford And James Martin School Institute of Particle Therapy Cancer Research Institute, Wilkinson Building, Oxford Physics Bleddyn.Jones@rob.ox.ac.uk.

E N D
Towards a UK Charged Particle Research Facility Bleddyn Jones MD Gray Institute for Radiation Oncology and Biology, University of Oxford And James Martin School Institute of Particle Therapy Cancer Research Institute, Wilkinson Building, Oxford Physics Bleddyn.Jones@rob.ox.ac.uk
RBE, relative biological efficiency or effect, is ratio of doses of high LET and low LET radiation for same bio-effect Survival curves of mammalian cells after single exposure or fractionated irradiation, from E.Hall; Lippincott Co, 1994
Example of altered radiobiological behavior with high LET radiation: effect of growth rate Neutron RBE vs photons RBE according to the doubling time of human lung metastasis. Battermann et al. Eur J Cancer 17:539-48, 1981
High LET radiations and hypoxic cells N2 02 Human renal cells T1, hypoxia, normoxia; from Broerse & Barendsen, IJRB, 13:559, 1967
LET, OER & RBE (EBR en France) Tubiana, Dutreix et Wambersie, Hermann ed, 1986
LET and RBE initially increases linearly with LET, increased probability of strand breakage, many of which will lead to a lethal event, As ionisations become closer, yield of Strand Breaks (SB) reduces, and same principles apply at higher levels e.g. chromosomal damage track 1 2 3 4 5 6 7 SB 0 1 1 2 2 1 0
Fit to Barendsen’s kidney T cell data using mono-energetic particles using a UK Poisson statistical model by estimating initial slope and max value, entire LET – RBE relationship can be predicted Zone where High LET questionable
PCT to treat a wide spectrum of cancers using protons and light ions • Depth in tissue range 2 – 30 cm • Higher dose rates than previously achieved with synchrotrons that might allow rapid scanning Bragg peak frequency with small spot sizes 1mm+ • Energy selection • Compact size, shielding and cost • Controllability in a hospital setting
NHS requirements • Some proton therapy centres (? by 2013) will probably use conventional accelerator technology • High throughput • Acceptable cost/benefit ratio compared with conventional radiotherapy and per life year of benefit • Competition from entire health budget • Implications on other parts of service…diagnostic radiology, pathology, medical physics etc • Travel and accommodation
Research Requirements • Relative roles of protons and ions • Choice of various ions, He, Ne etc in terms of physical and biological properties • Integration with other forms of cancer treatment…surgery, drug therapies, ultrasonics, laser, etc [combinations give best results] • Optimum fractionation • Optimum safety, use of RBE, • Patient selection: biological predictive assays • Physics dose computation……across UK • Patient experience • Quality of life /cure /cost outcomes
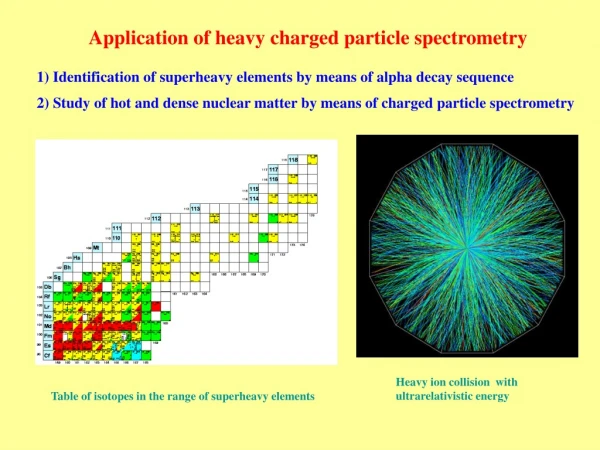
Small peripheral T1, T2 stage lung cancer now treated in single session in NIRS Japan with < 7% loss in respiratory function vital capacity/Tco HIMAC : Treatment Room
Gantries Three fixed fields • Angles critical • Patients can be rotated on vertical axis only on flat couch; horizontal axis rotation leads to long delays and possible inaccuracies • Various combinations fixed and movable gantries • Isocentric concept: 4-6 fields in 10-20 minutes using Linear accelerators • A cost effective solution is proton gantries + fixed fields for C ions….but +/- 200 shifts required to reduce skin entrance dose esp. for large dose per fraction. • Can more flexible fixed beams with variable geometry be designed; insert additional magnet/change/reversal or modification of electromag. field at final portion ??? Couch rotation allowed Versatile ‘fixed’ field
Isocentricity: use constant distance from treatment source to isocentre –a defined {x, y, z} point within tumour target Set up P1 % Depth dose inversely proportional to source skin distance for divergent beams, so before computers used in depth calculation a constant source skin distance was preferred X cm P2 Distance of P1, P2 and P3 to isocentre is constant = x cm Set up accuracy better than previous system of constant source to skin distance; also faster. P3
Adenoidcystic Ca Lacrimal Gland – 72 CGE – dose tracking of cranial nerves
1 year 3 years 4 years 5 years New indications? Kidney Cancer : Stage I, TIa N0 M0National Institute of Radiological Sciences, Chiba, Japan carbon ions, 80GyE / 16fr. /4wks 治療前 Can radical surgery be avoided? Better cancer screening might create extra need to use physics solutions
Some possible Gantry combinations1. not possible to transfer between rooms for same treatment fraction (time elapsed for DNA repair) 2. phases allowed where volumes change, room changes then permitted.3. e.g. start with 2 fixed fields, finish later with 3 or 4 angled fields4. Second cancers (due to radiation) should depend on reduction of volume of low dose exposure in patient
Imaging : need verification of beam placement Low Voltage XRays better bone definition MV beams poor bone definition Optical systems with same divergence geometry can be used as far as skin X-ray film or image intensifier screen X-rays bone Simple x-ray systems can be used to determine daily set up w.r.t bony anatomy 3-D CT/MRI fusion has made this easier, with recognisable reconstructions of anatomy, but more challenges in proton/ion therapy…use proton radiography, soft x-rays, MV x-rays, nuclear activation and PET analysis?
Nuclear activation detection sensitivity and specificity • Should detectors increase is sensitivity, it may be possible not only to confirm tumour position relative to beam, but also study temporal changes in tumour physiology….e.g. oxygen content, volume, blood flow and if deposition of heavy metals has occurred [Pl, Gad, Au, In ]. • Knowledge of rate of change/directionality rather than absolute values would be useful. • Confirmation of dose/inaccuracies…..and their subsequent (non-linear) correction
protons C ion Chemotherapy pulses These plots represent two extremes: there will inevitably be intermediate rates of change in perfusion
Post operative radiation • Treatment to a zone of risk, defined anatomically and not to a distinct cancer Where is the cell……….where is the electron ? Probabilities….back to Schroedinger et al. ?
New accelerator technologies e.g. NS- FFAG and lasers capable of very high dose rates and different spot scanning dose painting patterns/methods • Statistics of obtaining reliable reproducible dose distributions/overlaps/smaller spot sizes/over and underdose. • Over dose allowed in tumour; not in NT /OAR • Mobile tumours; probability of miss enhanced or reduced? • Radiobiology
Some Basic Radiation Biology • Expected Lethal events per cell= • Surviving Fraction= • Tumour cure probability= • Repopulation term
How can we picture BED ? Dose for same effect in single fraction Dose for same effect in four fractions BED DOSE Surviving Fraction Iso-effect level Imagine the dose to be given in infinitely small fractions with no curvature to slope Single fraction
BED - The Concept • Represents total dose if given in smallest fraction size
BED equations for high LET radiations RBE is dL/dH The RBE at low dose The RBE at high dose Low doses or if changes very little with increasing LET relative to Assuming that high LET changes in are relevant at high doses Jones, Carabe and Dale BJR 2006 – adapted for treatment interruption calculations
High LET radiobiology – general principles Using BED equation with RBEmax and RBEmin; low
MV X-rays and protons > 100 MV C ions RBE >> 1-5 RBE ≈ 1 or 1.1 Neutrons
Fractionation (according to Newton or Liebniz) T f(n-1), where f is average inter-fraction interval; Eliminate n and T in Then differentiate and solve (dE/dT)=0 to give max cell kill for constant level of normal tissue side effect defined by the BED. Also for more sparing forms of radiation d=gz, where z is dose to tumour and d to normal tissue
The solution when plotted shows that z’ : • Increases as g is reduced, as with a better dose distribution • Reduces as f is shortened, • Increases with K (for rapidly growing tumours) • Increases as / of cancer approaches that of the normal late reacting tissues [OAR]. • With an increase in RBE, z falls, but all above features the same
High LET optimum dose per fraction Even for protons, treatments might be accelerated; Germany 19# Japan 16, 10, 4, 1 #
Space flights and large doses per fraction ! Prospects for long term survival of humans/cells in space will depend on improved knowledge of low and high LET radiation effects and their reduction. Poissonian modification of LQ model to compensate for 2nd, 3rd hits Cell experiment range Modelling range ?
LEM-local effect model • Calculates lesion number in a region of nanometre scale • Amorphous track structure model assumed • Uses low LET survival curve (LQ model) • Assumes straight line survival curve for low LET at high dose
MKM-microdosimetric kinetic model • Modified dual radiation action theory by Hawkins • SF=exp[-(0+.z*1D)D - D2] • z*1D Dose mean specific energy corrected by saturation effect [can be measured by a Rossi counter] • 0 the radiosensitivity at LET~0. • Use Kiefer-Chatterjee track structure model.
MKM and LEM are roughly equivalent in LET regions used in heavy ion therapy and for fractionated (low) doses • Both refer to surviving fractions down to 10-4. • This is the range of in vitro survival curves • Tumour control needs 10-8 to10-10 range • Further extension required to both models • GSI fractionation has so far been 19 fractions in 19 days – but now dooing boosts of 1-4 fractions after IMRT. • Japanese experience showed anomalous results at 1 fraction.
Clinical Cancer sites See Jones B, Clinical Oncology, 2008 Large research portfolio on clinical applications, relationship with other cancer therapies etc particularly possibilities of priming a cancer with drugs prior to elimination of cancer cell population by particle therapy • Breast • Prostate • Lung • Oesophagus • Brain & Spine • Head, neck • Thyroid • Gynaecology • Liver upper/Abdomen • Limbs • Palliation of metastatic cancer
Models of Tumour Hypoxia – iterative DailyFlux of cells Repopulating Oxic cells Cell death Quiescent Hypoxic cells Radiosensitivities modified by hypoxia Radiosensitivities not modified by hypoxia Initial conditions and variables: hypoxic fraction, reoxygenation rate, OER, repopulation rates, radiosensitivities and mean inter-fraction interval. Model repeats every day until TCP > 0.05. Modified from Scott (1988); alternative is to use analytical models with integration of effective OER with time to give average values. Results very similar.
Example of iterative loop in ‘Mathematica’ Nox = nox Exp[ -list d- list d^2 + 0.693 f /list ] Nhyp = nhyp Exp[ -listd/q- listd^2/q^2]; Ntot = nox + nhyp; Tcp = Exp[-ntot]; n = n+1; Reox = x nhyp; ntot = nox + nhyp; nhyp = nhyp – xnhyp - ynhyp; Nox = nox + reox Heterogeneity is included by having long lists of separate tumours each with different , , and w, the cell repopulation parameter.
SLOW RE-OXYGENATION Modelled dose responses for 250 different tumours with initial hypoxic fraction of 15% and 1% reoxygenation per day A : x-rays 2 Gy, 5 times per week, B : x-rays 1.4 Gy, 10 times per week. C : carbon ions (dose equivalent Gray, RBE=3) 5 times per week at 2.1 Gy-equivalent fractions, reduced OER value =1.5 assumed. D : carbon ions delivered in 6 Gy-equivalent fractions
Photons (x-rays) at 2 Gy per fraction Or, carbon ions at 6 Gy per # Or X-rays to 40 Gy in 20 fractions plus 6 Gy carbon X-ray and carbon more ‘effective’ than either alone
Full Economic Cost • Cost of treatment per fraction (n) + fixed costs of treatment planning etc • Cost of treatment failure, where failure probability = (1-TCP) • Cost other salvage therapies and or supportive care • Studies done for breast, head and neck and medulloblastoma, chordoma. • SCOPE for modelling optimum dose per fraction or fraction number in context of particle therapy, taking into account RBE, normal tissue sparing etc.
Dose rate effect modelling • Classical dose rate effect is linked to parameter • But must also be affected at very high dose rates: G2 repair, relationship between dose rate and low dose radiosensitivity needs investigation • LET and RBE produces much greater increase in than in .
Dose rate effects on tissues Depends on tissue/cells as to where saturation of effect occurs. Also, some earlier work back in 1960 -70s showed local oxygen depletion at very high dose rates; might affect outcomes for protons. ROB could re-look this in a more modern setting Generally speaking at higher LET, the dose rate effect is less significant…the solid curve shown would be almost flat. M=marrow, G=gut, E=skin L=lung…….no error bars!
UK Carbon ION ModellingCarbon ions for early lung cancer (Japanese experience): using Monte Carlo computer simulation of hypoxic and oxic (repopulating) with re-oxygenation flux, reduced oxygen dependency of ion cell kill and typical RBE. (see chapters on Oxygen Effect and High LET Radiotherapy in Radiobiological Modelling in Radiation oncology: eds Dale and Jones Published by British Insitite of radiology, London, 2007) Model accounts for single fraction deviation from present Japanese model
Malignant Induction Probabilities with compensation for fractionation and high LET Let x be proportion of chromosome breaks cell kill, and (1-x) cancer P[malignant ch. break] P[cell survival due to lethal ch. breaks]
Beam – multiple components, elastic, non elastic, nuclear fragmentation, -rays, neutrons [detectors, MC simulations] Target configurations at sub-cellular level [molecular and cell biology] ? Micro-dosimetry RBE……….varies between RBEmax at zero dose to RBEmin at very high dose Bio-effect models outcomes Dose prescription