Download
1 / 11
250 likes | 3.35k Views
TEMPOROMANDIBULAR DISLOCATION. BY DR. MANISHA MISHRA. TMJ. The temporomandibular joint (TMJ) is the articulation of the temporal and mandibular bones

E N D
TEMPOROMANDIBULAR DISLOCATION BY DR. MANISHA MISHRA
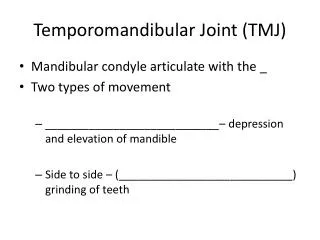
TMJ • The temporomandibular joint (TMJ) is the articulation of the temporal and mandibular bones • TMJ dislocation occurs when the condyle travels anteriorly along the articular eminence and becomes locked in the anterior superior aspect of the eminence, preventing closure of the mouth. • This results in stretching of the ligaments, and is associated with severe spasm of the muscles that open and close the mouth (ie, the masseter, internal pterygoid, and temporalis) . • The resultant trismus prevents the condyle from returning to the mandibularfossa
Causes: • Deep yawning • Prolong Dental procedures • Airway manipulation particularly in an anaesthetised patient. • Dislocation can occur during laryngoscopy, transoral fiberoptic bronchoscopy and intubation.
Clinical features: • TMJ dislocation may occur with trauma, but most often follows extreme opening of the mouth during yawning, laughing, singing, vomiting, or dental treatment . • Dislocation also can result from dystonic reactions to drugs . • Symmetric mandibular dislocation is most common, but unilateral dislocation with the jaw deviating to the opposite side also can occur. • TMJ dislocation is painful and frightening for the patient.
On examination: • The patient is unable to close the mouth and there is excessive salivation . • A depression may be noted in the preauricular area. • Palpation of the TMJ reveals one or both of the condyles trapped in front of the articular eminence and spasm of the muscles of mastication. • Patients prone to mandibular dislocation include those with an anatomic mismatch between the fossae and articular eminence, weakness of the capsule and the temporomandibular ligaments, and torn ligaments. • Patients who have had one episode of dislocation are predisposed to recurrence .
Diagnosis: • The dentist bases the diagnosis on the position of the jaw and the person's inability to close his or her mouth. • Radiographs of the TMJ are not always necessary, but should be obtained to exclude condylar fracture if the dislocation is related to trauma • The problem remains until the joint is moved back into place. However, the area can be tender for a few days.
Treatment : • The muscles surrounding the temporomandibular joint need to relax so that the condyle can return to its normal position. • Many people can have their dislocated jaw corrected without local anesthetics or muscled relaxants. However, some people need an injection of local anesthesia in the jaw joint, followed by a muscle relaxant to relax the spasms. • The muscle relaxant is given intravenously (into a vein in the arm). Rarely, someone may need a general anesthetic in the operating room to have the dislocation corrected. • In this case, it may be necessary to wire the jaws shut or use elastics between the top and bottom teeth to limit the movement of the jaw.
To move the condyle back into the correct position, a doctor or dentist will pull the lower jaw downward and tip the chin upward to free the condyle . • The doctor or dentist then guides the ball back into the socket. • After the joint is relocated, a soft or liquid diet is recommended for several days to minimize jaw movement and stress. • People should avoid foods that are hard to chew, such as tough meats, carrots, hard candies or ice cubes, and advice not to open their mouths too widely.
Prevention: • TMJ dislocation can continue to happen in people with loose TMJ ligaments. To keep this from happening too often, dentists recommend that people limit the range of motion of their jaws, for example by placing their fist under their chin when they yawn to keep from opening their mouths too widely. • Conservative surgical treatments can help to prevent the problem from returning. • Some people have their jaws are wired shut for a period of time, which causes the ligaments to become less flexible and restricts their movement. • In certain cases, surgery may be necessary. • Eminectomy removal of the articular eminence so that the ball of the joint no longer gets stuck in front of it. • Another procedure involves injecting medications into the TMJ ligaments to tighten them.
Prognosis: • The outlook is excellent for returning the dislocated ball of the joint to the socket. • However, in some people, the joint may continue to become dislocated , If this happens, needs surgery.